Excerpt
Table of contents
1 INTRODUCTION
2 ANATOMY OF THE SHOULDER COMPLEX
3 BIOMECHANICS
4 REVIEW OF LITERATURE
5 SHOULDER ARTHROSCOPY: BASIC PRINCIPLES OF POSITIONING, AND PORTAL ANATOMY
6 ARTHROSCOPIC ANATOMY´OF SHOULDER JOINT
7 MATERIAL AND METHODS
8 AGE AND SEX
9 DISCUSSION
10 SUMMARY AND CONCLUSION
11 REFERENCES
1 INTRODUCTION
Shoulder articular cartilage has very limited intrinsic repair properties, hence any derangement in and around shoulder joint leads to early degenerative changes, pain, instability and limitation of movements.
With improvements in technology and instrumentation, arthroscopy has become the primary treatment modality for many shoulder disorders. Compared with open techniques, arthroscopy has smaller incisions and damage to deltoid muscle is very less, improved intra-articular visualization, less pain, and faster postoperative recovery.
The indications for shoulder arthroscopy include labral lesions and instability, impingement syndrome, rotator cuff tear, synovitis, osteoarthritis, calcific tendonopathy and other pathologies.
An analysis of data from the UK Hospital Episode Statistics database concluded that there is 7.5fold increase in the number of patients undergoing arthroscopic acromioplasty over a 10year period, from 2,523 patients in 2000–2001 to 21,355 patients in 2009–2010(135). They also concluded that in 2002–2003 only 4.6% arthroscopic acromioplasty procedures per 100,000 individuals were perform, whereas by 2009–2010 that number had risen to 83.6%. Shoulder arthroscopy in USA describes a similar trend, with a 250% increase (from 29.9 to 102.2 patients per 100,000 of the population) observed in New York between 1996 and 2006; notably, the overall increase in orthopedic surgery was only 78% during the same period.
A broad range of shoulder pathologies has become amenable to arthroscopic diagnosis and treatment. In addition to its diagnostic role, arthroscopic procedure is developed for the treatment of impingement syndrome, rotator cuff tear, Glenohumeral instability with bone loss or without bone loss and Labral lesion. In contrast to the knee, for which option of surgical arthroscopy came few years after the ability to perform diagnostic arthroscopy, diagnostic and surgical arthroscopy in the shoulder evolved concurrently.
One of the benefits of shoulder arthroscopy has been ability to define both intraarticular and subacromial anatomy. Normal anatomic variation can be better appreciated and greater diagnostic can be achieved.
Arthroscopic subacromial decompression become the most important treatment for the impingement syndrome. Studies have shown that Arthroscopic Sub Acromial Decompression (ASD) had a better effect because patients could spend less time in the hospital and could return to their activities of daily living and work more quickly, less pain and improvement in range of motion.
Arthroscopic capsular release become mainstay treatment for frozen shoulder. In many long-term follow-up study (average 7 years) of patients who underwent arthroscopic capsular release showed that the early gains in range of motion, improvement in pain and function outcome. Shoulder motion was comparable to that of the unaffected shoulder at 1 year
Rotator cuff repair (RCR) has evolved considerably in the past decade, most notably with a shift away from open repair toward arthroscopic techniques. Jaicharan J. Iyengar(142) et al in 2014 concluded that there is 353% increase in arthroscopic rotator cuff repair from 2001 to 2009 in Florida and the rate of increase in arthroscopic RCRs significantly outpaced the rate of decrease in open RCRs.
Arthroscopy for the evaluation and treatment of shoulder instability has been evolving. The ability to see intraarticular pathology such as hill sachs, bankart, ALPSA, on track and off track lesion helps in defining the complexity of instability and its treatment. Arthroscopic shoulder stabilization offers numerous advantages over open procedures. It provides circumferential visibility of the unopened shoulder joint and avoids complications related to subscapularis incision. It has been shown to decrease intraoperative blood loss, surgical time, postoperative narcotic use, and the length of the patient’s hospital stay. Finally, arthroscopic shoulder surgery is associated with an easier functional recovery, faster return to athletic activities, maximal preservation of joint motion, and improved cosmetics.
Arthroscopic remplissage has become the most popular treatment for engaging Hill-Sachs lesions. Remplissage is French for “filling” and is a unique procedure in which a bony defect is replaced with soft-tissue coverage. A recent study shows improved outcomes, minimal losses of external rotation, and few complications with arthroscopic remplissageand it is the safest and most stable option.
Before the advent of the shoulder arhroscopy, the role of the superior portion of the glenoid labrum in producing shoulder symptomatology was unclear.Current data indicate that arthroscope is most important tool in diagnosis and treating SLAP lesion.
Other types of shoulder pathology are also proving amenable to arthroscopic treatment like removal of loose body, debridement of distal clavicular osteophytes, subcricoid impingement, supraclavicular nerve release, rotator cuff calcification, and treatment of synovial diseases of shoulder.
In this study we have evaluated and assessed the role of arthroscopy in different shoulder pathologies, both diagnostic and therapeutic.
2 ANATOMY OF THE SHOULDER COMPLEX
The shoulder joint consist of the clavicle, scapula, and humerus; the glenohumeral joint and acromioclavicular (AC) joints that unite them.
GLENOHUMERAL JOINT
The glenohumeral joint is a synovial ball and socket joint between the humeral head and the glenoid fossa of the scapula. The shallowness of the glenoid fossa and the disproportionate size and lack of congruency of the articular surfaces make the joint inherently unstable. Stability is primarily dependent on capsuloligamentous structures and the musculotendinous cuff.
Glenoid
Inferior to the acromion, the flat scapula thickens to form the glenoid .The spinoglenoid notch separates the base of the acromion from the glenoid. The total surface area is three to four times smaller than that of the humerus. The glenoid faces laterally, being 10"to 15"superiorly tilted relative to the medial border of the scapula.
Relative to the plane of the scapula, the glenoid surface is nearly perpendicular and there is retroversion of an average of 7.4" with an incidence of 75% or anteversion of an average of 2" to 10" with an incidence of 25%.
Glenoid Labrum
The glenoid labrum is a ring of triangular shape in section overlying the peripheral circumference of the glenoid with its free rim projecting into the joint. It consists of dense fibrous tissue.
It is attached to the glenohumeral ligaments and blends superiorly with the origin of the long head of the biceps tendon at the supraglenoid tubercle.
Its function is to increase congruity, generating a suction effect and enhancing stability of the glenohumeral joint.
Glenohumeral Joint Capsule
The capsule of the glenohumeral joint has a large volume of normally about 10 to 15 mL and twice the surface area of the humeral head.
On the inside, it is covered with synovium; on the outside, rotator cuff tendons protect the capsule on all but the inferior aspect. The capsule begins at the border of the labrum, is attached to its outer surface, and is anchored onto the bone of the glenoid neck. It extends superiorly to the coracoid process and in varying length along the biceps tendon into the intertubercular groove.
The glenohumeral ligaments reinforce the joint capsule. They are an abrupt thickening of the inner layer with organized collagen bundles in the frontal plane. A thickening of middle layer reinforces the axillary pouch. Contrary to the anterior joint capsule, the posterior is quite thin.
Glenohumeral Ligaments
The coracohumeral ligament originates from the base and lateral border of the coracoid process and runs transversely to the greater tuberosity. Its anterior border is distinct medially and merges laterally where as its posterior border is indistinct.
The superior glenohumeral ligament is variable in size and origin. It arises from the anterior labrum, sometimes as far superior as the long head of the biceps tendon and sometimes as far inferior as the middle glenohumeral ligament or in between.
The middle glenohumeral ligament shows the largest variation in diameter. It can be as thin as the capsule or as thick as the subscapularis tendon. It originates from the anterior labrum or glenoid neck to insert into the lesser tuberosity underneath the subscapularis tendon with which it is mingled.
The inferior glenohumeral ligament is thicker than the rest of the capsule, although variable in size and attachment site. Its structure resembles a hammock consisting of a prominent anterior band, a posterior band, and the axillary pouch in between.
Humeral Head
The articular surface has an ovoid shape facing medially, superiorly and posteriorly .The humeral head is inclined about 130" relative to the shaft with 30" of retrotorsion relative to the condyles of the elbow.
The intertubercular groove lies 30" media170 or 9 mm anterior to the central axis of the articular surface. It is bordered by the lesser tuberosity anteriorly and by the greater tuberosity posteriorly. The transverse ligament bridges the inter-tubercular groove proximally to act as a retinaculum for the long head of the biceps tendon.
Distally the subscapularis tendon inserting onto the lesser tuberosity forms the floor of the sheath. The supraspinatus tendon inserting onto the greater tuberosity forms its roof. The depth of the inter-tubercular groove seems to play a role in the pathogenesis of long head of the biceps tendinitis by more or less exposing the tendon to an impingement process.
There are three facets on the greater tuberosity: the superior, the middle, and the inferior .The supraspinatus muscle inserts onto the superior facet and the superior half of the middle facet. Anterior fibers of the supraspinatus tendon mingle with the subscapularis tendon fibers. Posteriorly the infraspinatus tendon attaches to the middle facet, covering the posterior border of the supraspinatus tendon. The teres minor tendon inserts onto the inferior facet.
Scapulo-humeral Muscles
Supraspinatus. The supraspinatus muscle takes fleshy origin in the supraspinatus fossa to have a tendinous insertion onto the greater tuberosity. The muscle belly has a fusiform shape with a thick tendinous core, the intra- muscular tendon, located in the anterior third.
Approximately 70% of the muscle fibers attach o the intramuscular tendon, whereas 30% attach directly to the extramuscular tendon. The supraspinatus is part of the force couple to stabilize the glenohumeral joint by compression and initializes elevation.The suprascapular nerve (C4-6) supplies innervation.
Infraspinatus. The infraspinatus muscle takes fleshy origin in the infraspinatus fossa and scapular spine to insert with a flat tendon onto the middle facet of the greater tuberosity.
The infraspinatus muscle stabilizes the glenohumeral joint by resisting posterior and superior translation and generates 60%of the overall external rotation force. The suprascapularnerve (C4-6) supplies innervation.
Teres Minor. Origin of the teres minor muscle is the lateral border of the scapula and the infraspinatus fascia, and its fleshy insertion is located inferior to the infraspinatus muscle on the inferior facet of the greater tuberosity.
The teres minor muscle acts as stabilizer of the glenohumeral joint by resisting posterior and superior translation and generates 45% of the total external rotation force. The posterior branch of the axillary nerve (C5-6) supplies innervation.
Subscapularis. The subscapularis muscle takes fleshy origin in the subscapularis fossa and inserts onto the lesser tuberosity.
The subscapularis sends fibers of its tendinous insertion across the intertubercular groove to form the floor of the bicipital sheath. As the only component of the anterior rotator cuff, it stabilizes actively the glenohumeral joint by resisting anterior and inferior translation and acts as a strong internal rotator. It is considered to be a passive stabilizer, too, because of the dense collagen structure of its tendon and its fusion with the middle and inferior glenohumeral ligament.
Two branches of the subscapular nerve (C5-8) for the superior and inferior portion of the muscle supply innervation.
Deltoid. The deltoid muscle is composed of the clavicular part originating from the lateral clavicle, the acromial part from the acromion, and the spinal part from the scapular spine. Their common insertion is the deltoid tubercle on the humerus.
The deltoid is the most important abductor of the glenohumeral joint. Although the acromial portion is the strongest one and starts the movement, the clavicular and spinal portions participate at higher degrees of abduction. The axillary nerve (C4-5) innervates the deltoid.
Biceps. The long head of the biceps muscle has its origin at the supraglenoid tubercle. Ensheathed by the synovial membrane, it runs intrarticularly on top of the humeral head to exit the joint capsule through the intertubercular groove.
The short head of the biceps originates from the coracoid process. Both heads have a common insertion onto the tuberosity of the radius laterally and onto the ulnar fascia of the forearm medially. Although it acts as a stabilizer of the humeral head, main function is to affect elbow flexion and forearm supination. The musculocutaneous nerve mainly supply biceps muscle (C5-6). Triceps. The long head of the triceps originates from the infraglenoid tubercle and the inferior labrum to insert in common with both other heads onto the olecranon. The long head participates in extension and adduction of the glenohumeral joint, whereas the main function is the extension of the elbow. Radial nerve mainly supplies triceps muscle.
Coracobrachialis. The coracobrachialis muscle originates with the short head of the biceps from the coracoid process to insert onto the anteromedial surface of the central humerus. It participates in flexion and adduction of the glenohumeral joint.
3 BIOMECHANICS
Motion
The humeral head is convex in the anterior-posterior direction than in the superior-inferior. The motion of the glenohumeral joint is basically ball-and- socket in nature.
During active and passive arm elevation, the superior-inferior translation of the humeral head is only 0.3 to 0.35 mm in normal shoulders. “Anterior-posterior translation is substantially larger. The head translates anteriorly 3.8 mm on average during flexion, translates posteriorly 4.9 mm during extension, and translates 4 mm during horizontal extension.
Larger translations in the anterior-posterior direction than in the superior-inferior direction occur as a result of the bony configuration of the glenoid because it is more concave in the superior-inferior direction than in the anterior- posterior direction.
Stability
Ligaments. The superior glenohumeral ligament is an anterior stabilizer" and an inferior stabilizerinthehangingarm position .The major role of the middle glenohumeral ligament is anterior stabilization with the arm in aductionupto3 0 t o 4 5 " of abduction.This function is apparent in 90" of abduction with the arm in neutral rotation but not in external rotation. It is also an inferior stabilizer with the arm in adduction.
The inferior glenohumeral ligament is the most important anterior stabilizer with the arm in abduction and external rotation, the position of anterior dislocation. The function is by its anterior band and the axillary pouch but not by its posterior band. The posterior band is a posterior stabilizer with the arminflexionandinternal rotation, or in 90" of abduction. With abduction and external rotation, the anterior band fans out to support the humeral head, whereas the posterior band becomes cordlike. The opposite happens in internal rotation.
The coracohumeral ligament (CHL) is known to be an inferior stabilizerwith the arm in adduction. It functions as an inferior stabilizer and tightens in external rotation.
A rotator cuff interval lesion is clinically apparent as inferior instability with the arm in internal rotation but not in external rotation.The rotator interval capsule indirectly stabilizestheshoulderinferiorlybymeans of maintaining the negative intra-articular pressure.
In external rotation, the CHL prevented inferior instability even after the interval capsule was sectioned. The rotator interval capsule alsoprovides posterior stability.
Glenoid Concavity. The glenoid fossa has a concavity, which centers the humeral head on the glenoid. It is deeper in the superior-inferior direction than in the anterior-posterior direction.The humeral head is more stable in the superior-inferior direction than in the anterior- posterior direction.
When the head is compressed onto the glenoid fossa, the force necessary to dislocate the head is approximately 60% of the compressive force (stability ratio) in the superior-inferior directions and 35%in the anterior-posterior directions.
Labrum. The function of the labrum is to increase the stability of the humeral head on the glenoid socket by increasing the depth of its cavity. After removal of the labrum, the stability ratio decreases by 20% on average.
Scapular Inclination. Shoulder was stabilized inferiorly by the scapular inclination angle in the hanging arm position. In shoulders with multidirectional instability, the scapula is less abducted during arm elevation than in healthy shoulders. Inferior instability as part of multidirectional instability can thus be explained by the lack of the stabilizing effect of scapular inclination.
Intra-articular Pressure. The capsule surrounds the shoulder joint, and the pressure inside the capsule is negative when the arm is in hanging position. With a downward load applied to the arm, the negative pressure in- creases, preventing the inferior translation of the humeral. The negative pressure provides inferior stability with the arm in abduction.
Muscles. Muscles stabilizes the joint by the following five mechanisms (1) bulk of the muscle generate passive tension(2) contraction causing compression of the articular surfaces (3) joint motion that secondarily tightens passive ligamentous constraint (4) barrier effect of the contracted muscle (5) redirection of the joint reaction force to the center of the glenoid surface by coordination of muscle activity.
Rotator Cuff. The subscapularis was described as the most important active and passive anterior stabilizer among the rotator cuff muscles. subscapularis, supraspinatus, and infraspinatus and teres minor equally contributed to anterior stability of the abducted shoulder with the arm in neutral and in external rotation. With the arm in 90 degree of flexion, the subscapularis is the primary posterior stabilizer.
The rotator cuff muscles usually function together. Inman et al introduced a concept of a force couple in the frontal plane consisting of the deltoid and supraspinatus muscles as elevators and inferior portions of the rotator cuff muscles as depressors.
Saha et al described the force couple in the horizontal plane, the subscapularis muscle act anteriorly and infraspinatus and teres minor muscles act posteriorly.
If the rotator cuff muscles are loaded simultaneously, the humeral head is stabilized in the superior-inferior direction as well as in the anterior-posterior direction.
Rupture of the long head of the biceps tendon, leads the humeral head translates superiorly during arm abduction.Stabilization by the long head of the biceps depends on the integrity of the superior labrum. After creating a superior labral lesion, the stabilizing function of the biceps becomes less efficient as a result of the lax labrum and the elongated tendon.
Moment Arn. Kuechle et al studied and measure the moment arms of the rotator cuff muscles during abduction and adduction with help of electropotentiometer . According to his study, the supraspinatus is the most efficient elevator, and the teres minor is the most efficient depressor of the rotator cuff muscles throughout the entire range of motion. The infraspinatus changes from being an elevator to being a depressor, and the subscapularis changes from being a depressor to being an elevator with increasing elevation angle.
During rotation with the arm at the side, the infraspinatus and the teres minor were the most efficient external rotators. The subscapularis was the most efficient internal rotator followed by the pectoralismajor, latissimusdorsi, teres major, and anterior deltoid.
During rotation with the arm abducted, the most efficient external rotators were the teres minor followed by infraspinatus, where as the most efficient internal rotators were the subscapularis.
4 REVIEW OF LITERATURE
History of shoulder arthroscopy
Burman et al in 1931(143) is credited with first arthroscopic examination of shoulder.
Andren et al 1965(143) has been credited for first clinical use of arthroscopy in the treatment of frozen shoulder.
Wantanabe et al in 1978(143) describe the anterior and posterior shoulder portals and in 1979 discuss the arthroscopic finding in shoulder pathology.
Conti et al in 1979(25,143) described the use of an anterior arthroscopic cannula to perform capsular release on 18 patients with frozen shoulders.
Wiley and Older(143,136) developed arthroscopic technique and their results with various shoulder pathology published in 1980.
Jhonson et al in 1980(143, 57) gave the details about intra-articular shaver.
Gross and Fitzgibbons in 1985(143,42) modified this straight lateral decubitus position by tilting the patient 20 to 30 degrees posteriorly, which places the glenoid surface parallel to the floor. They reported three advantages of this modification: (l) less traction, decreasing the risk of neurapraxia of the brachial plexus; (2) accentuation of tears of the glenoidlabrum because they are pulled away from their beds instead of in line with them; and (3) improved arthroscopic access to the inferior third of the glenoid labrum and capsule.
Warren et al in 1986(143) advocate beach chair position.
Ellman and paulos et al in 1985-1986(143, 35) performed arthroscopic subacromial decompression.
Gartsman et al in 1988(143) demonstrated the anatomic efficiency of subacromial decompression and excellent visualization of the rotator cuff.
Andrews et al 1984(5,143) describes the role of arthroscopic management of partial tear rotator cuff.
Snyder and Pattee et al in 1988(128,143) presented arthroscopic classifiacation and treatment of Rotator cuff tear.
Arthroscopic management of Recurrent shoulder instability
Johnson and Detrisac (1980)(57,144) performed the first arthroscopic shoulder stabilisation procedure, using a capsular stapling technique.
Morgan 1987.(94,144) Suggested Arthroscopic labralfixation bytransglenoidsutures, he published the first series of Bankart repairs with in 1987.
Caspari et al in 1987(19,144) described a transglenoid suture technique that allowed the surgeon to advance and adjust tension in the capsuloligamentous structures.
Wiley 1988(136,144) described a similar approach using rivets for labral fixation. The use of suture anchors in Bankart repair appeared shortly after in publications by Snyder and Wolf in 1990 followed by non-threaded bio-absorbable tacks.
Harryman et al(144,45) proposed suture-only labral repair in 1994.
Neviaser et al 1993(144,99), described a lesion that differed from the one reported by Bankart, because the anterior scapular periosteum did not rupture and allowed thereby the labro-ligamentous structures to displace medially and rotate inferiorly on the scapular neck; this “anterior labrol-igamentous periosteal sleeve avulsion” (ALPSA) was recognized as a cause of anterior instability of the shoulder. The same author distinguished this lesion from the glenolabral articular disruption (GLAD), a similar post-traumatic nding not associated with signs of anterior instability.
In 1993, Wolf et al(144,139,138) described in detail the humeral avulsion of glenohumeral ligaments as a possible cause of anterior instability in patients without a demonstrable Bankart lesion and proposed an arthroscopic repair technique.
Further studies recognized several different injury patterns of the capsule and the glenohumeralligaments, later summarized in the West-Point classification. Glenoid avulsions of the glenohumeral ligaments were described by Wolf 5 years after their humeral counter- parts. This author popularised also the arthroscopic remplissage (originally described as an open procedure) to address the humeral bony Hill–Sachs lesion.
Warner et al(135,144) introduced cannulatedbioabsorbable tacks for Bankart repair in 1995 . These implants had a relatively short learning curve, avoided posterior glenoid penetration, and were resorbed after 4 weeks.
Abbildung in dieser Leseprobe nicht enthalten
Figure : showing bioabsorbable tacks
GeoffroyNourissat et al 2006(144,104) first performed an arthroscopically assisted mini-open Bristow–Latarjet procedure in cadaveric specimens, suggesting that this could be a safe and effective procedure with certain advantages over an all open technique.
Nobuyuki Yamamoto, EijiItoi et al in 2007(145,144) gave the concept of the “glenoid track” with “on track” and “off track” Hill–Sachs lesions.
Laurent Lafosse et al in 2007(71,144) performed Arthroscopic Latarjet procedure.
Alessandro Castagna et al in 2007(145,20) gave concept of Arthroscopic intervention for shoulder microinstability.
Boileau, Laurent, and EttoreTaverna 2007, Italian surgeon has reported an arthroscopic bone graft procedure using tricortical iliac crest autograftfixed with a button technique.
EttoreTaverna, Markus Scheibe(144,124) et al in 2008 performed Arthroscopic bone graft procedure (Eden procedure)
Markus Scheibel et al 2008(144,124) uses a similar technique by biocompression screws for graft fixation.
Freedman et al in 2004(39); they concluded that the arthroscopic group had a significantly higher rate of recurrent instability (20.3 vs 10.3 %) with poorer post-operative scores than the open repairs.
Petrera et al (113) Found similar re-dislocation and re-operation rates in arthroscopic suture anchors operations compared to open Bankart repair. However, a statistically significant difference in favor of the arthroscopic group was found when studies after 2002 were considered (2.9 vs. 9.2 %)
Chin khoonTan,IinigoGuisasola,BhuvaneshwarMachani2006(146) concluded that[i] after conducting a prospective study in 130 patients with a follow up of 2 years, Arthroscopic Bankart repair and stabilization with absorbable and non absorbable suture anchors with redislocation rate of 6% and no significant difference between usage of absorbable suture anchor to Nonabsorbable suture anchor.
Boileau P in 2006(13,14) concluded that the treatment of traumatic recurrent anterior shoulder instability, patients with bone loss or with shoulder hyperlaxity are at risk for recurrent instability after arthroscopic Bankart repair. At least four anchor points should be used to obtain secure shoulder stabilization. Ninety-one consecutive patients underwent arthroscopic stabilization for recurrent anterior traumatic shoulder instability. At a mean follow-up of thirty-six months, fourteen patients (15.3%) experienced recurrent instability: six sustained a frank dislocation and eight reported a subluxation. The mean delay to recurrence was 17.6 months. The risk of postoperative recurrence was significantly related to the presence of a bone defect, either on the glenoid side (a glenoid compression-fracture; p = 0.01) or on the humeral side (a large Hill-Sachs lesion; p = 0.05). The number of suture-anchors was critical: patients who had three anchors or fewer were at higher risk for recurrent instability (p = 0.03).
Abbildung in dieser Leseprobe nicht enthalten
Figure Drawings demonstrating the optimal placement of anchors on the glenoid rim to recreate normal articular concavity.
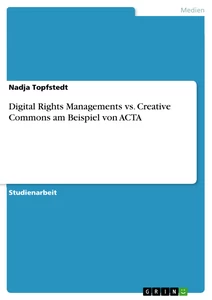
Tim R. Lenters, MD, Amy K. Franta, MD, Fredric M. Wolf, PhD, Seth S. Leopold, MD, and Frederick A. Matsen III, MD(147) did a systemic review in 2007 and concluded that that arthroscopic approaches are not as effective as open approaches in preventing recurrent instability or enabling patients to return to work. Arthroscopic approaches resulted in better function as reflected by the Rowe scores in the randomized clinical trials. The study design and the arthroscopic technique had substantial effects on the results of the analysis.
Figure (147): Standardized mean differences (SMD) in Rowe scores as shown by subgroup analysis of study quality with use of a fixed-effects model.
Abbildung in dieser Leseprobe nicht enthalten
Figure:(147) Relative risk (RR) of recurrent instability as shown by subgroup analysis of arthroscopic technique with use of a fixed-effects model. n/N = number with recurrent stability/number in study.
J. Hobby, D. Griffin, M. Dunbar, and P. Boileau 2007(148) did a systematic review and metaanalysis of 62 studies including 3044 arthroscopic operations concluded that the failure rates are less in arthroscopic stabilization using suture anchors and bioabsorbabletacs, compared to arthroscopic stabilization with staples and transglenoid suture technique arthroscopic anterior stabilization using the most effective techniques has a similar rate of failure to open stabilization after 2 years of.
Harris et al. 2012(44) done a systematic review of 26 studies dealing mainly with post-traumatic anterior instability in young male patients, without significant glenoid bone loss, demonstrated that arthroscopic suture anchor and open Bankart techniques yield similar long-term clinical outcomes, with no significant difference in the rate of recurrent instability or rate of return to sport follow up.
Randelli et al 2012(120) gave the risk factors for recurrence after arthroscopic Bankartrepair: age below 22 years; male gender; a greater number of preoperative dislocations; participation in competitive sports; repair with fewer than three anchors; use of knotless anchors; the presence of an ALPSA lesion or bony deficiency of the glenoid or humerus.
Joshua D. Harris et al 2013(44) done a systemic review and included 26 studies and he compare and analyse the long-term (minimum of 5 years) clinical and radiographic outcomes in patients who have undergone open or arthroscopic Bankart shoulder stabilization. Analyze and compare the long-term (minimum of 5 years) clinical and radiographic outcomes in patients who have undergone open or arthroscopic Bankart shoulder stabilization. No of patient in his study where 1781 out of which no of male 1097(81%) and number of female where 264(19%). Right shoulder involve in 53% of the patient and left shoulder in 47%.Dominant shoulder in 61% and non dominant in 39%. Length of follow-up is done for 11.3 +/- 6.5 years. Number of patient who underwent open Bankart repair where 731 and arthroscopic Bankart repair where done in 584 patient.). He found that there was no significant difference in recurrence of instability with arthroscopic (11%) versus open (8%) techniques.
Furthermore, there was, no significant difference was observed between arthroscopic suture anchor repair (87%) and open repair (89%). There was no significant difference in the rate of postoperative osteoarthritis between arthroscopic suture anchor and open Bankart repair (26% and 33%, respectively). There was no significant difference in Rowe or Constant scores between groups.
Peter N. Chalmers et al in 2014(149) conduct a systematic review of overlapping meta-analyses comparing open and arthroscopic shoulder stabilization. Studies published prior to 2007 concluded that open stabilization provided lower recurrence rates than arthroscopic stabilization, the, and studies published after 2008 concluded that open and arthroscopic stabilization provided equivalent results.
Tim R. Lenters in 2015(147) studied and compares arthroscopic and open surgical repairs for the management of anterior glenohumeral instability. He found that arthroscopic repairs were associated with significantly higher risks of recurrent instability, recurrent dislocation, and a reoperation. When considered alone, arthroscopic suture anchor techniques were associated with significantly higher risks of recurrent instability. Arthroscopic approaches were also less effective than open methods with regard to enabling patients to return to work and/or sports
Concepts of arthroscopic management of recurrent anterior glenohumeral joint instability with bone loss
Piasecki DP et al(114) stated thatbone loss in the context of glenohumeral instability includes glenoid, humeral or combined defects. Glenoid defects are mainly located in the anteroinferiorglenoid between the 2 and 6 o’clock position.
Provencher MT(117) et al in 2012concluded that Humeral osseous defects in the context of anterior glenohumeral instability, referred to as Hill-Sachs lesions, occur where the posterolateral aspect of humeral head abuts against the anterior glenoid
Edwards et al (2003)(33) reviewed plain films of chronic anterior shoulder instability and found an osseous lesion of glenoid in 78% and humeral impaction fracture in 73%. A series of two-dimensional (2D) computed tomography (CT) scans has shown glenoid bone loss in 86% of patients with glenohumeral instability.
Sugaya et al 2003(130) found a glenoid osseous defect in 50% of patients with recurrent shoulders instability. The presence of a Hill-Sachs lesion consistent with humeral bone loss in recurrent shoulder instability is estimated to be between 38% and 88%
Balg et al (2007)(7) gave the instability severity index score, which identified six risk factors that may predict failure of an arthroscopic soft tissue Bankart repair. These included age < 20 years, participation in contact sports, competitive level, shoulder hyperlaxity, a Hill-Sachs lesion, and a loss of contour of the glenoid rim. Scoring > 6/10 on this scale predicted a 70% failure of Bankart repair in such patients.
Burkhart et al 16 concluded that when bone loss is more then 25% there is 67% recurrent instability rate in such patients undergoing only soft tissue Bankart repair in contrast to 4% in those without bony deficiency.
Lafosse et al 2010(70) concluded that no recurrence in 96 patients treated with an arthroscopic Latarjet with 91% of patients reporting an excellent subjective outcome on Disabilities of Arm, Shoulder and Hand score.
Ilia Elkinson ett al in 2012 done a experimental study and concluded that In this experimental model, addition of remplissage provided little additional benefit to a Bankart repair in specimens with a 15% Hill-Sachs defect, and it also reduced specific shoulder motions. However, Bankart repair alone was ineffective in preventing engagement and recurrent dislocation in specimens with a 30% Hill-Sachs defect. The addition of remplissage to the Bankart repair in these specimens prevented engagement and enhanced stability, although at the expense of some reduction in shoulder motion.
Horst K et al 2014(59) shown that the presence of an isolated glenoid or humeral defect increases the chances of an associated bipolar defect by a factor of 2.5 to 11.
Buza et al. 2014 (55) conducted a systematic review of patients who underwent a remplissage procedure in association with a Bankart repair for patients who had instability and a humeral head osseous defect. The studies included 167 patients (mean age, 27.5 years) with a mean follow-up of 26.8 months (range, twelve to forty-three months). Patients had a frequency- weighted mean adjusted Rowe score of 36.1 preoperatively compared with 87.6 postoperatively (p < 0.001). In the studies with motion measurements, shoulder motion was not affected postoperatively (p > 0.05); mean forward elevation changed from 165.7° preoperatively to 170.3° postoperatively, and mean external rotation changed from 57.2° to 54.6°. Nine of 167 shoulders experienced an episode of recurrent glenohumeral instability (overall recurrence rate, 5.4. He concluded that Postoperative clinical outcome scores were generally good to excellent following arthroscopic remplissage. No studies indicated a significant loss of shoulder motion following the procedure. The failure rate following Hill-Sachs remplissage compared favorably with previously published rates for patients without clinically important Hill-Sachs lesions who underwent arthroscopic Bankart repair alone. The overall complication rate across the studies was low.
Longo et al. 2014(78) analysed studies reporting on various interventions for instability with humeral bone. They concluded that combination of remplissage and Bankart procedures was associated with a lower rate of recurrence when compared with Bankart repair alone and that remplissage was the safest technique for the management of patients with shoulder instability with humeral bone loss.
Longo UG and Loppini M et al 2014(79) systematic review of 46 studies involving 3211 shoulders demonstrated similar lower recurrence rates of instability following bone block procedures compared with Bankart repair. Higher rates of arthritis were demonstrated following the Eden–Hybinette procedure. Furthermore, an important reduction in external or internal rotation and elevation was observed in all studies that evaluated range of motion after bony transfer surgery.
Bhatia S. et al 2014 The low rate of recurrent instability for these procedures has been corroborated by other studies and reviews, particularly when accounting for the fact these surgeries are frequently per- formed in cases where there may be more severe bone loss or in the revision setting.
Di Giacomo G in 2014 concluded that Co-existing osseous defects of the humerus and glenoid are termed bipolar lesions. Bipolar lesions can be defined as “on-track” or “off track,” which describes the degree to which the humeral Hill- Sachs defect engages the glenoid defect in a position of 90 degrees of abduction and external rotation of the shoulder.
PietroRandelli et al in 2016 did a systemic review study and concluded that A Hill-Sachs lesion could not be confirmed as a statistically significant negative prognostic factor after arthroscopic Bankart repair.
Thomas C. Alexander et al in 2016(131), hepercutaneously place 2 suture anchors, which require no additional suture passing across the tissue, to create a double pulley technique, filling the defect with posterior capsule and rotator cuff. Therefore, the Hill-Sachs defect becomes extra-articular, eliminating the potential engagement of the anterior glenoid and contribution to recurrence of instability. This technique is applicable broadly for most Hill-Sachs lesions that need addressing. By not having to pass or shuttle any suture through tissue after anchor placement and by eliminating the necessity to go subacromially to retrieve or tie suture, the technique saves time and improves reproducibility. The compression of tissue into the Hill Sachs surface area also is improved by double-reinforced suturing through the double-pulley technique. The combination of these advantages creates a sound and efficient technique for remplissage.
Arthroscopic management of Frozen shoulder
Conti (1979)(25) described the first arthroscopic release.
Inferiorly from medial to lateral in an anterior-to-posterior direction. Posterior capsular release can then be performed by placement of the camera anteriorly and by use of a posterior working portal).
Ogilvie-Harris and Myerthall1997(106) reported on their technique of anteroinferiorcapsulotomy in diabetic patients. They used a shaver to perform the capsulotomies, even in the axillary recess. In the interval area, only the synovitis was addressed. Nevertheless, 13 of 17 patients returned to full external rotation postoperatively.
AbdelsalamEid (2012)(3) reported that the use of miniopen Coracohumeral ligament release and manipulation of the shoulder as a safe and simple method of treating idiopathic frozen shoulder that could be performed as a quick procedure under short duration anaesthesia obtaining a significant improvement of shoulder function. A case series including fifteen patients (19 shoulders) with idiopathic frozen shoulder operated by this technique is described.
Hugh M.J. Le Lievre et al (2012)(47) reported that Patients with idiopathic adhesive capsulitis treated with a circumferential arthroscopic capsular release of the glenohumeral joint. At a mean follow-up of seven years (range, five through thirteen years), forty-three patients (forty-nine shoulders) had significant improvement with regard to pain frequency and severity, patient-reported shoulder function, stiffness, and difficulty in completing activities compared with the findings at the initial presentation (p < 0.001) and the one-year follow- up evaluation (p < 0.01 to p < 0.001). Shoulder motion also improved (p < 0.001) and was comparable with that of the contralateral shoulder.
Laurent Lafosse et al in 2012(69) studied arthroscopic 360° capsular release for the treatment of global frozen shoulder. Ten patients with global adhesive capsulitis were prospectively evaluated. All patients had not improved after undergoing a minimum of 6 months of physiotherapy, and 5 received intra-articular injections of steroids.
The mean follow-up was 42 months (range, 18 to 90 months), and the mean Constant score improved from 21 to 72 (P.01). Preoperative abduction improved from a mean of 40° to 165°, elevation improved from 55° to 175°, and external rotation improved from 6° to 58°. The visual analog scale pain score improved from 7 to 1.6, and all patients reported an excellent outcome after surgery. There were no complications particularly regarding axillary nerve injury, fracture, or infection.
R. Dattani et al in 2013(119) study was done to assess the functional and health-related quality of life outcomes following arthroscopic capsular release (ACR) for contracture of the shoulder. Between January 2010 and January 2012 68 patients who had failed non-operative treatment including anti- inflammatory medication, physiotherapy and glenohumeral joint injections for contracture of the shoulder were enrolled in the study. He concluded that ACR resulted in a highly significant improvement in the range of movement and functional outcome, as measured by the Oxford shoulder score and EuroQol EQ-5D index.
Mohammad H Ebrahimzadeh et al in 2014(91) done a prospective study, 80 patients (52 females and 28 males) with recalcitrant frozen shoulder underwent arthroscopic release and patients follow-up was 47.2±6.8 months. The VAS score, constant shoulder score, Rowe score, UCLA shoulder score, and DASH score showed significant improvement in shoulder function after surgery, and shoulder range of motion improved in all directions compared to pre-operation range of motion.
Smith CD et al(127) 2014 performs Arthroscopic capsular release for idiopathic frozen shoulder in 136 patients.. At 12 months, the Oxford shoulder score was calculated, and pain and range of motion were assessed. Fifty per cent achieved good pain relief within a week and eighty per cent within six weeks of arthroscopic capsular release. The mean preoperative visual analogue scale pain score was 6.6 and the mean postoperative score was 1.0. The mean time to achieving good pain relief was 16 days following surgery. No patient could sleep through the night prior to surgery while 90% reported having a complete night's sleep at a mean of 12 days after surgery. The mean postoperative Oxford shoulder score was 38/48 and the mean improvement was 19.2.
Michal Waszczykowski et al in 2014(90) assess the impact of arthroscopic capsular release of frozen shoulder on muscular strength of the operated shoulder and comparison of the results obtained with non-affected shoulder. All the patients underwent arthroscopic superior, anteroinferior, and posterior capsular release. After at least two-year follow-up, measurement of muscular strength of abductors, extensors, and external and internal rotators of the operated and nonaffected shoulder, as well as determination of range of motion (ROM) and function (ASES) in the operated and nonaffected shoulder, was performed. Measurement of muscular strength in the patient group did not reveal statistically significant differences between operated and nonaffected shoulder. The arthroscopic capsular release does not have significant impact on the decrease in the muscular strength of the operated shoulder.
[...]
- Quote paper
- Ajit Singh (Author), 2017, Arthroscopic Management of Common Shoulder Pathologies, Munich, GRIN Verlag, https://www.grin.com/document/919839
Similar texts



Publish now - it's free

Comments