Excerpt
Table of content
List of Abbreviations
List of formulas
List of figures
List of tables
1. Introduction, Objective, Questions
1.1 Introduction
1.2 Objective
1.3 Research questions
2. Theoretical background
2.1 Definitions
2.1.1 Haemodialysis
2.1.2 Classification of vascular access
2.1.3 Ultrasound and doppler technology in medicine
2.1.4 Quality of life concept
2.2 Historical development and technology of doppler sound
2.2.1 Historical development
2.2.2 Technology of ultrasound
2.3 Empirical findings on ultrasound-guided venepuncture
3. Methodical approach
4. The use of ultrasound-guided shunt cannulation
5. Economic evaluation of different types of care
5.1 Costs and revenues in dialysis therapy
5.1.1 Costs of therapy from payer’s perspective
5.1.2 Costs of therapy from hospital perspective
5.1.3 Costs of therapy from dialysis centre perspective
5.1.4 Opportunity costs of dialysis centres
5.2 Revenue elements
5.2.1 Revenue of hospitals
5.2.2 Revenue of dialysis centres
5.3 Cost-benefit analysis
5.3.1 Cost-benefit analysis from payer’s perspective
5.3.2 Cost-benefit analysis from hospital perspective
5.3.3 Cost-benefit analysis from dialysis centre perspective
6. Expected outcome
6.1 Use of ultrasound technology for payer and service providers
6.1.1 Use of ultrasound technology from payer’s perspective
6.1.2 Use of ultrasound technology from hospital perspective
6.1.3 Use of ultrasound technology from dialysis centre perspective
6.2 Shunt cannulation, shunt survival and Quality of life
6.2.1 Cannulation quality and shunt survival
6.2.2 Quality of life
7. Summery and reference to research questions
7.1 Monetary benefit
7.2 Acceptance by patients
7.3 Cannulation quality and shunt survival
8. Critical view and further research needs
9. VI Bibliography
Annexes
List of Abbreviations
Abbildung in dieser Leseprobe nicht enthalten
List of figures
Figure 1: Distribution (%) of patients by dialysis treatment types 2006
Figure 2: Diagram of hemodialysis
Figure 3: Radiocephalica (RC) AVF
Figure 4: AVF on the proximal forearm
Figure 5: AVF in the elbow
Figure 6: AVG on the forearm
Figure 7: Subclavian and jugularis catheters
Figure 8: Port system
Figure 9: Emergency vehicle with special signal
Figure 10: How Piezoelectricity Works
Figure 11: Principle of the transducer
Figure 12: Sound methods of ultrasonic technology
Figure 13: Calcification with acoustic shadow
Figure 14: Cyst with sound amplification
Figure 15: Economic evaluation procedures of a comparative nature
Figure 16: Cost diagram insurance provider
Figure 17: Effects of the length of stay in the revenue and cost comparison
Figure 18: 5-year reduction in ultrasonic puncture costs
Figure 19: Puncture haematoma
Figure 20: Shunt occlusion by thrombus
Figure 21: Research flowchart ultrasound-guided shunt puncture
List of tables
Table 1: Costs from the point of view of insurance providers in the inpatient are
Table 2: Settlement items by EBM 2016
Table 3: Costs per case 2016 or a hospital
Table 4: Costs of one dialysis unit
Table 5: Revenues of the hospital for cases 1 to 3
Table 6: Revenues of a dialysis unit for cases 1 to 3
Table 7: Cost Analysis from the perspective of Cost Providers
Table 8: Costs and revenue overview for hospitals and dialysis facilities
Table 9: Graduation of the weekly flat rate and costs of the dialysis facility
Table 10: Costs and revenue of ultrasound use per year
Table 11: Empirical findings on ultrasound-supported puncture
Table 12: Use of ultrasound-guided shunt puncture
1. Introduction, Objective, Questions
1.1 Introduction
In February 2016, approximately 100,000 people in Germany were affected by chronic kidney disease according to projections of health insurance company data. Of these, 80,000 were in a dialysis program and 20,000 were in post-transplant care (cf. Albers, 2016).
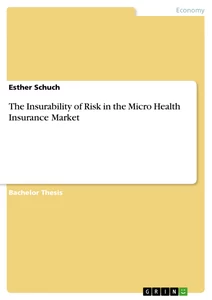
Of the approximately 80,000 dialysis patients, 5 % are treated with peritoneal dialysis, approximately 1 % undergo dialysis therapy as home haemodialysis in their own homes. 95 % of all patients undergo haemodialysis therapy 3 times a week for 4 to 5 hours in one of the dialysis centres. A graph from the 2006 QuaSi Kidney Report illustrates this in Figure 1. For cost reasons, the collection of data after this survey was terminated. However, the percentage distribution has not changed much to date (cf. Frei; Schober-Halstenberg, 2008, p. 16).
Abbildung in dieser Leseprobe nicht enthalten
Figure 1: Distribution (%) of patients by dialysis treatment types 2006 Source: QuaSi-Niere-Bericht 2006, p. 16
A sufficient access to the vascular system is necessary for haemodialysis treatment. It represents the "lifeline" for the patient and is also his "Achilles' heel". A well-functioning vascular access is of essential for haemodialysis treatment and influences the dialysis quality and thus the patient's quality of life. The best vascular access is the arterio-venous fistula (AVF) (cf. Parisotto; Pancirova, 2015, p. 28).
With a frequency of 3 dialysis per week and 2 punctures per dialysis, every haemodialysis patient receives at least 375 punctures, faulty punctures and additional dialysis at 52 weeks per year. Based on a waiting time of 10 years before transplantation, that is 3,750 punctures per patient. Often the punctures are accompanied by pain or associated with fears of faulty punctures and haematomas. In addition, there is the fear of the failure of the dialysis shunt and an inpatient stay to restore functionality. A long-life span of the AVF thus ensures the survival of the patients.
1.2 Objective
The health economic relevance of this topic results firstly from the trans-sectoral structure of our healthcare system. This results in different responsibilities and billing systems for outpatient and inpatient services. The players in the individual sectors are trying to optimise their own budgets without achieving an overall economic optimisation. The evaluation of costs and benefits is therefore very important, especially when introducing new forms of care or using new technologies (cf. Schöffski; Fricke, 2008, p. 82).
Secondly, 80,000 dialysis patients incur costs of EUR 3.2 billion annually for the health system of the Federal Republic of Germany. This amounts to EUR 40,000 per dialysis patient per year (cf. DGfN, 2014). Total health costs in 2014 amounted to 328 billion euros (cf. Mannschreck, 2016). This means that 80,000 dialysis patients - 0.1 % of the total population - are responsible for almost 1 % (0.967 %) of healthcare costs in 2014. 33 % of inpatient treatment of dialysis patients is due to problems with vascular access (cf. Albers, 2014, p.1).
For this reason, international associations and professional societies pay special attention to the AVF. A well-functioning vascular access should fulfil the following criteria: visible, palpable, of appropriate size and free of infection signs. This enables adequate haemodialysis (cf. Parisotto; Pancirova, 2015, p. 28).
That is precisely where the difficulties are. On the one hand, the increase in the number of elderly people is leading to an increase in cardiovascular complications and vascular calcification; on the other hand, the number of people with diabetes has been rising for years. A late complication of this " public disease " is kidney failure requiring dialysis (cf. Potthoff et al., 2015, pp. 39 and 48). This complicates the creation of functional vascular accesses that satisfy the criteria of the European Dialysis and Transplant Nurses Association/European Renal Care Associations (EDTNA/ERCA) (cf. Parisotto; Pancirova, 2015, p. 28) and the requirements of the Interdisciplinary Working Group Dialysis access (IAD) and the vascular access for haemodialysis: Interdisciplinary Working Group (GHIA), of minimal vessel diameters. (cf. Hollenbeck et al., 2009, p. 3; Parisotto; Pancirova, 2015, p. 64 f.).
The graduation of the weekly flat rate in 2013, the associated increase in the ratio of care per nurse (1:6 in Germany, Switzerland and Scandinavia 1:4), the use of less qualified personnel (medical specialists) and the increase in the dialysis program for very old multimorbid dementia patients only vaguely indicate the explosiveness that also results for a safe puncture of dialysis shunts. Chronically ill people require not only technical treatment care, but also holistic care that lasts for years. The obligation to undergo dialysis means a lifelong dependence on the dialysis machine, restrictions in nutrition, drinking volume, secondary diseases and the ingestion of many drugs. All this requires high professional competence of the team of dialysis centres (cf. Gerpheide, 2013, 2f.).
1.3 Research questions
The following questions are answered in this thesis:
1. Does the use of ultrasound-guided shunt cannulation offer specific monetary benefits for the payers and for individual dialysis units?
1. Is the acceptance of shunt cannulation by patients improved when using ultrasound technology?
2. Is the use of ultrasound associated with an improvement in cannulation quality and longer shunt survival?
The thesis gives an overview of dialysis and the status of ultrasound-guided shunt puncture. In addition to the requirements for personnel and technology, the use of this method is considered from a cost-benefit perspective in relation to
- re-creation and revision of vascular accesses
- the economic consequences for the payers,
- loss of revenue for the individual dialysis unit,
- preserving a high cannulation quality of the vascular accesses
and
- Quality of Life of the patients.
After the introduction, objectives and questions in the first chapter, the definition of technical terms for further understanding of the text is given in the second chapter. The historical development of ultrasound technology is described in a short summary. Empirical findings on the technique of ultrasound-supported venepuncture will be described with the help of literature. They have been the basic for the further development of the shunt cannulation procedure.
The third chapter describes the methodical procedure for data acquisition and evaluation.
The fourth chapter contains the current state of knowledge on the application of ultrasound-guided shunt cannulation.
In Chapter 5, the treatment forms are evaluated economically. A cost-benefit analysis is performed on the basis of the costs and revenues of dialysis therapy from the perspective of both service providers and cost units.
Chapter 6 deals with the expected results in terms of the benefits of ultrasound-guided shunt cannulation for cost units and service providers, for shunt cannulation and shunt survival as well as for the quality of life of patients.
Chapters 7 and 8 conclude the work with a summary and a reference to the research questions, a critical examination and further research needs.
2. Theoretical background
2.1 Definitions
For a better understanding of the relationships between dialysis therapy, shunt puncture and quality of life of dialysis patients, technical terms will be explained in more detail here. These include "haemodialysis", the "classification of vascular access" for dialysis therapy, the term "ultrasound", and the World Health Organization (WHO) definition of "Quality of Life".
2.1.1 Haemodialysis
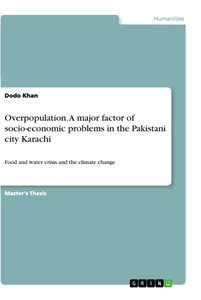
Haemodialysis or blood washing refers to a form of renal replacement therapy, which also includes peritoneal dialysis and kidney transplantation. It becomes necessary when the function of the body's kidneys like: excretion of metabolic toxins and water, maintenance of the acid-base balance, hormone production for blood formation and blood pressure reduction, is no longer sufficient. The affected people develop uraemia with progressive loss of function and different symptoms: toxic symptoms up to coma, polyneuropathy, pericarditis, cardiomyopathy, gastroenteritis, overhydration, hypertension, anaemia and osteopathy, pruritus. These symptoms can be reversed or alleviated by dialysis therapy, depending on the severity, type and duration (cf. Borger, 1997, p. 22f). Figure 2 Illustrated the principle of haemodialysis.
Abbildung in dieser Leseprobe nicht enthalten
Figure 2: Diagram of haemodialysis Source: Nowack, Birck, Weinreich, 2003, p. 118
2.1.2 Classification of vascular access
Until 2009, there was a heterogeneous landscape in Germany about dialysis access in terms of the name, its plant and its significance for renal replacement therapy. On the initiative of the German Association for Clinical Nephrology, the boards of directors of various specialist associations joined forces in 2008 to form the GHIA. The guideline "Vascular access to haemodialysis" was developed from its interdisciplinary recommendations (cf. Hollenbeck; Mickley; Brunckwall et al., 2009).
This guideline is based on the "European Best Practice Guidelines on Vascular Access" (cf. Tordior; Canaud; Haage et al., 2007, p. ii88ff). Afterwards, haemodialysis accesses are classified as first to third choice accesses:
Access of the first choice:
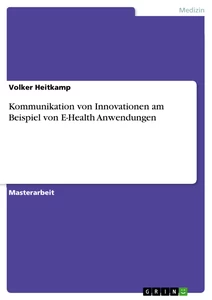
Creating a native AVF - The Radiocephalica (RC) AVF on the wrist is the first option. If matured adequately, it can be used for years with minimal complication rate, revisions and interventions. The long-term function rate is 65-90% after one year and 60-80% after two years, with a simultaneous low incidence rate of thrombosis (0.2 events per patient per year) and infections (2%). One disadvantage is the rate of early occlusion of 5 - 30 % (cf. Hollenbeck; Mick-ley; Brunkwall et al., 2009, p. 161).
Abbildung in dieser Leseprobe nicht enthalten
Figure 3: Radiocephalica (RC) AVF Source: aucklandvascular.com
AVF on the proximal forearm can be applied as anastomosis between the arteria (A.) radialis and the vein (V.) cephalic on the middle forearm up to the elbow if a wrist near AVF is not possible in inadequate vascular conditions (cf. Hollenbeck; Mickley; Brunkwall et al., 2009, p. 161).
Abbildung in dieser Leseprobe nicht enthalten
Figure 4: AVF on the proximal forearm
Source: vascularclinic.com
AVF in the elbow generates a high blood flow and is indicated when the peripheral vessels are too fragile for proximal fistulas. AVFs enable highly efficient dialysis with a low incidence of thrombosis and infection. The main disadvantages of high shunt flows are the development of hand ischaemia and the risk of heart failure in predisposed patients (cf. Hollenbeck; Mickley; Brunk-wall et al., 2009, p. 161).
Abbildung in dieser Leseprobe nicht enthalten
Figure 5: AVF in the elbow
Source: dialyseshunt.com
Access of the second choice:
The second choice are implants made of polyurethane, polyester (Dracon®) and polytetrafluoroethylene. Implants (AVG) are used when the creation of AVF is no longer possible. In the long term, stenosis of the venous anastomosis often leads to shunt thrombosis. At 30 - 40 %, the primary openness rate after two years is significantly lower than that of native AVF. Second choice approaches also include transposition of the saphenous vein or superficial femoral vein to form a native AVF in the femur (cf. Hollenbeck; Mickley; Brunkwall et al., 2009, p. 161).
Abbildung in dieser Leseprobe nicht enthalten
Figure 6: AVG on the forearm
Source: vascularclinic.com
Access of the third choice:
According to the GHIA, there are only a few indications for tunnelled Central Venous Catheters (CVC) as permanent dialysis access. These include serious ischemia of the upper limbs caused by the first two types of dialysis access, severe heart failure and disseminated carcinoma.
CVC for chronic dialysis treatment should be used as the last option (degree of evidence III), as can be read in Hollenbeck et al. If an acute, possibly reversible need for dialysis is assumed, transient central venous catheters must be used (degree of evidence III) (cf. Hollenbeck; Mickley; Brunkwall et al., 2009, p. 173).
Abbildung in dieser Leseprobe nicht enthalten
Figure 7: Subclavian and jugularis catheters
Source: trianglevascular.com
The application of port catheter systems offers cosmetic advantages, but the infection rates are like those of central venous catheters. In addition to the increased risk of infection (sepsis 1 - 5 %), port dysfunction also plays a decisive role in dialysis effectiveness (cf. Hollenbeck; Mickley; Brunkwall et al., 2009, p. 173).
Abbildung in dieser Leseprobe nicht enthalten
Figure 8: Port system
Source: trianglevascular.com
In this paper, literature on ultrasound-guided cannulation of native AVF and AVG is considered. In central venous catheters, ultrasound support plays a central role only for access placement (degree of evidence II) (cf. Hollenbeck; Mickley; Brunkwall et al., 2009, p. 173).
2.1.3 Ultrasound and doppler technology in medicine
The word "sonography" is a Latin "sonare" - sound. The term "ultrasound" is used synonymously (cf. Hildebrandt (ed.), 1994, p. 1433).
Ultrasound is used in medicine as an imaging, non-invasive method in diagnostics. Used as a pulse echo method, a piezoelectric crystal (transducer) generates sound waves and simultaneously acts as a sound receiver. The generated sound waves are in the high frequency range, above 1 kHz. The time difference between emitting and receiving the reflected sound waves is proportional to the depth of a reflecting layer. The echo pulses are converted back into electrical pulses, amplified and displayed on the monitor. Here a distinction is made between A-scan, B-scan and M-scan method or mode, description in Chapter 2.2.2 (cf. Hildebrandt (Ed.), 1994, p. 1592f.).
In addition to the pulse echo method, there is also the continuous sound method or Doppler method. The crystal transmits continuous ultrasonic waves of constant frequency. When a sound beam hits a moving interface, some of the waves are reflected at a different frequency. This is called the Doppler effect. This interference produces a low-frequency sound, which is made audible by amplification. This method enables the monitoring of the shunt flow and can be used for the detection of stenosis in shunt monitoring and for diagnostics before surgical interventions (cf. Hildebrandt (Ed.), 1994, p. 1594).
2.1.4 Quality of life concept
Quality of life can be classified into general quality of life and health-related quality of life. Today's concept of health-related quality of life has developed from social science welfare and social indicators research and medical research (cf. Buddeberg, 2004).
The 1948 WHO definition of health as "[...] The state of complete physical, mental and social well-being and not only the absence of illness and handicaps" can be seen as a comprehensive view of health and illness (WHO, 1948).
There is no general definition of quality of life. The WHO defined the concept very broadly in 1997 (cf. WHO, 1997):
„ Quality of Life as individuals’ perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns. It is a broad ranging concept affected in a complex way by the person’s physical health, psychological state, level of independence, social relationships, personal beliefs and their relationship to salient features of their environment.”
Along with political stability and a person's level of education, health is a fundamental element of quality of life. Especially in chronically ill people, health comes to the foreground, and becomes decisive for the subjective definition of quality of life (cf. BN, 2014).
2.2 Historical development and technology of doppler sound
The following section gives a brief historical outline of the development of ultrasound technology up to its use for vascular punctures.
2.2.1 Historical development
The astronomer, mathematician and physicist Christiaan Huygens (1629 - 1695) described the wave theory of light in 1678, which is one of the physical foundations of Doppler technology. It describes the occurrence and propagation of waves. The Huygen principle means that every point of a wave front can be regarded as the starting point of a new wave (elementary wave). His findings are regarded as the basement for the wave optics (cf. Huygens, 1690).
After the biologist Lazzaro Spallanzani (1729 - 1799) presented his theory on the orientation of bats in 1795 (cf. Sales; Pye, 1974), Hamilton Hartridge (1886 - 1976) did not investigate the orientation by ultrasound emission and analysis of reflected sound waves until 1898 (cf. Starling, 1920). In 1938 the zoologist Donald Redfield Griffin (1915 - 2003) succeeded in transforming the ultrasound sounds of bats into the human ear (cf. Pierce, 1938, p. 454f).
The Austrian Christian Doppler (1803 - 1853), professor of mathematics and physics, described in his main work in 1842: "Über das farbbige Licht der Doppelsterne und einiger anderer Gestirne des Himmels" the Doppler effect, the dependence of the wavelength on the direction of propagation of a moving object (cf. Doppler, 1842, p. 465).
The frequency shift when a rescue vehicle passes by with a special signal, as can be seen in Figure 9, is an everyday phenomenon of the Doppler effect. With an approaching emergency vehicle with a special signal, a high-frequency sound with a high amplitude (volume) is perceived, whereas the sound of the approaching vehicle is perceived as low-frequency and quieter (low amplitude).
All empirical values and their practical applications follow the formula:
The Doppler frequencies measured in the ultrasonic frequency range from 1 kHz and at physiological flow rates ∆f lie in the hearing range from 50 Hz to 15 kHz and can therefore be perceived directly by the human ear as an audio signal.
Abbildung in dieser Leseprobe nicht enthalten
Figure 9: Emergency vehicle with special signal
Source: Schneider, 2016, p.4
In 1912, after the sinking of the Titanic, the physicist Karl Friedrich Alexander Behm (1880 - 1952) developed the echo sounder principle for watercraft to measure sea depths and detect obstacles. In 1917 the first pulse echo system for locating submarines was put into operation (cf. Klemm, 1955, p. 7f.).
From 1935, ultrasound energy was used in medicine to improve blood circulation in muscle tissue, to destroy tumours due to overheating and for two-dimensional imaging using the ultrasonic method. The first ultrasonic devices for material testing were used and made non-destructive material testing possible for the first time (cf. Hiedemann, 1939).
After the breakthrough in medical imaging in 1950 with the representation of interfaces inside the body, Hertz and Edler succeeded for the first time in 1953 in assigning structures of the moving heart to the "teeth" of the ultrasound image:
„Yet an M-mode echocardiogram was not a “picture” of the heart: it was a diagram that showed how the position of its structures changed during the cardiac cycle. “
(Durham, 2011, p. 1)
2.2.2 Technology of ultrasound
After technical progress made the use of ultrasound technology in medicine possible, more and more examinations and therapies were carried out.
Sound waves propagate in different frequency ranges. In human tissue sound continues at a speed of 1,540 m/s (cf. Schneider, 2016, p. 4).
A mechanical ultrasonic wave is created by converting an electrical voltage into vibrations of the small crystals. This principle is also known as the piezo effect and was first described by Jacques and Pierre Curie in 1880 (cf. Schneider, 2016, p. 5). Figure 10 shows the operating principle of a piezoelectric crystal. The atoms are arranged in such a way that the centres of gravity of the positive and negative charges of the crystal can move away from each other along an axis by compression. Depending on the type of crystal, there may be one or more such "polar axes" (cf. Mirwald, 2012, p. 2).
Abbildung in dieser Leseprobe nicht enthalten
Figure 10: How Piezoelectricity Works Source: Mirwald, 2012, p. 2
Medical ultrasound signals pass through various components before the examination area can be displayed as an image. The ultrasound transmitter is located in a transducer that the person being examined holds on to the part of the body to be sounded. In this transducer, ultrasonic pulses are generated from electrical pulses and conducted into the tissue via a contact medium. In shunt ultrasound, an alcohol-based skin disinfectant is used to perform a hygienic shunt puncture according to the hygiene guidelines for dialysis (cf. Spindler, 2016, p. 13 and 19). In a pulse-echo method (Figure 11), the ultra-sonic pulses are sent into the arm and reflected differently where they meet interfaces. The closer an organ/structure is to the transmitter; the earlier the reflected sound waves return to the transducer. The transducer also serves as a receiver, also known as a detector.
Abbildung in dieser Leseprobe nicht enthalten
Figure 11: Principle of the transducer
Source: Schneider, 2016, p. 5
The signals are converted into electrical voltage in the detector. For visualization, the signal must be changed: after the conversion of the negative voltage into positive voltage (rectification), closely spaced voltage peaks are connected (smoothing). This way, the signal can be displayed as stripes with light and dark sections. For a complete image on the ultra-sonic monitor, a large number (one hundred or more) of such strips are required. The frequency height determines the penetration depth into the tissue. Frequencies of 10 to 15 MHz with a penetration depth of 3 to 5 cm appear to be the most suitable for subcutaneous structures, such as those to be evaluated for shunt puncture with a linear transducer (cf. Schneider, 2016, p. 6, 10; cf. Morgenstern, 2013, p. 190).
Different transducers with different sonic procedures are used for ultrasound examinations. Medicine distinguishes between A-, B- and M-Mode. B-Mode, Brightness-Mode, is used for shunt examination and puncture. It represents interfaces in the tissue and allows the evaluation of the expansion of cavities in the depth. The echoes are displayed as individual pixels. The stronger the echo, the brighter the pixels.
The A-mode is used, for example, for cardiac ultrasound. It enables the display of amplitudes, like the electrocardiogram (ECG), down to deeper layers and thus the assessment of cardiac activity. With the M-Mode, Time-Motion-Mode, time sequences of ultrasound images can be displayed. This mode enables the one-dimensional representation of movement patterns on a time axis (flow velocity of blood in the vessel). Figure 12 illustrates the described (cf. Schneider, 2016, p. 7ff).
Abbildung in dieser Leseprobe nicht enthalten
Figure 12: Sound methods of ultrasonic technology
Source: Schneider, 2016, p. 7
The transmitted and received signals are subject to refraction and scatter due to the impact on different interfaces. Artefacts such as calcifications create a sound shadow. For the examiner, underlying structures can no longer be assessed, as can be seen in Figure 13. Another artefact can be seen in Figure 14. Here, a cyst filled with fluid under the shunt prevents the view of deeper structures. The sound amplification can be seen as a dense white surface (cf. Schneider, 2016, p. 6ff).
Abbildung in dieser Leseprobe nicht enthalten Abbildung in dieser Leseprobe nicht enthalten
Figure 13: Calcification with acoustic shadow Figure 14: Cyst with sound amplification
Source: Schneider, 2016, p. 8 Source: Schneider, 2016, p. 9
The following section gives an overview of the practical use of ultrasound technology for venepuncture in anaesthesia and emergency medicine.
2.3 Empirical findings on ultrasound-guided venepuncture
Kawamura, Okabe and Namikawa published their first publication on ultrasound-supported venepuncture in the "Japanese Journal for Parenteral and Enteral Nutrition" in November 1987 and reported on the subclavian vein puncture from an ultrasound perspective (cf. Kawamura, Okabe, Namikawa, 1987, p. 505f). With the improvement of the equipment technology, the method was also used more frequently. Reports can be found from the end of the 1990s, mainly in the field of emergency medicine. An overview of all the tests listed is given in Appendix 1, Table 11.
In 1999, Keyes et al. reported in the "Annals of emergency medicine" on the puncture of the brachial and basilica veins in patients with difficult peripheral vein conditions, with repeatedly necessary punctures of central veins, in an emergency room. They found the method safe and fast, combined with a high success rate (cf. Keyes et al., 1999, p. 711ff).
In 2003 Blaivas et al. published a study in the "Academic emergency medicine" on the position of the transducer during the puncture of dummies, for learning the technique. They concluded that the practitioners got faster a safe access to the exercise vessel if the transducer was placed transversely to the vessel (short-axis) (cf. Blaivas et al., 2003, p. 1307ff).
In 2005, Costantino et al. published in the "Annals of emergency medicine" their examination results for the comparison of conventional venepuncture with the use of ultrasound technology in patients with difficult venous conditions. In summary, the authors consider ultrasound-assisted puncture to be safer for patients with difficult puncture conditions than the conventional "blind" puncture method. With the new technology, they needed less time to establish secure access (cf. Costantino et al., 2005, p. 456ff).
In 2009, Stein et al published a study in the "Academic emergency medicine", which also dealt with ultrasound-assisted puncture of peripheral veins in patients with difficult vein conditions in an emergency room. The automobiles concluded that the puncture technique could neither increase the number of safe punctures nor shorten the puncture time. Patient satisfaction was also not significantly increased compared to conventional vascular puncture. The study could not support the superiority of ultrasound-supported venepuncture over the conventional puncture technique (cf. Stein et al., 2009, p. 581f).
In the American Journal of Emergency Medicine 2010, Stone et al. dealt with the question of the ultrasound probe orientation for finding the needle tip in the vessel - in the direction of puncture (long-axis) vs. across the direction of puncture, the vessel (short-axis). They concluded that the long-axis method was the method of choice for finding the needle tip. Complications in the placement of central venous catheters could be further reduced, which should be further investigated in future studies (cf. Stone et al., 2010, p. 343ff).
In 2011, Schoenfeld, Shokoohi and Boniface published in the "West Journal of Emergency Medicine" a prospective observation study on ultrasound-guided venous puncture in emergency patients with difficult vein conditions. The punctures were performed by 19 medical-technical assistants. They received theoretical instructions and practical training sessions on the use of the technique. All participating patients were asked for a 10-point catalogue on the evaluation of patient satisfaction (cf. Schoenfeld et al., 2011, p. 475ff).
In 2016, Song et al. published a randomised study on arterial puncture in children in the "European Journal of Anaesthesiology". The two techniques of "in-plane/long-axis" and "out-of-plane/short-axis" were compared in terms of safety and puncture duration up to a safe access. They concluded that regardless of the longer training in the "in-plane technique", there were no significant differences in the puncture time for both types of puncture until a secure access was established. However, the rate of back wall injuries was lower in the "in-plane technique" (cf. Song et al., 2016, p. 1ff).
In 2010 and 2012, educational films on puncture of the jugular vein and peripheral venepuncture were made available online in "Videos in clinical medicine". The authors are Ortega et al. and Joing et al. (cf. Ortega et al., 2010; Joing et al., 2012).
All studies (except Stein et al., 2009) see ultrasound-assisted venepuncture as a safe and rapid procedure for patients and users to place a vascular access in difficult vascular conditions. She's the standard in Anglo-American emergency rooms. Theoretical and practical training is considered essential for mastering the technique. This laid the foundation for the use of ultrasound technology for shunt puncture in the dialysis facilities, initially by medical personnel and later also by trained specialist nurses.
3. Methodical approach
This chapter describes the methodical procedure for creating the work in more detail. The research flow diagram for literature on ultrasound-controlled shunt puncture is exemplarily documented in Appendix 2.
The basic methodology of the work is a structured literature analysis. The research was conducted in PubMed, DIMDI, EuCliD®, Cochrane Library, publication lists of the professional associations of nephrology, on the Internet pages of the professional groups of nephrological care and doctors as well as on grey literature from congresses and conferences, both nationally and internationally. The following terms were used in both German and English for the search: „haemodialysis, cannulation, cannulation techniques, vascular access, ultrasound guided, dialysis quality, patient’s outcome, cost analysis of haemodialysis access, quality of life “. To perform a comprehensive search, several search queries, separated according to the classification topics, were necessary. The search terms were varied, combined, linked with "and" or "or", truncated and other database aids used to optimize search results. New search approaches resulted additionally from the source and literature information of the evaluated finds.
Overall, 83 publications were identified for ultrasound-guided shunt puncture in PubMed for the period 1993 to 2016. 80 articles were excluded because they had no direct reference to the search criteria.
An article from 1997 was identified in the Cochrane Library. He treats the puncture of a femoral vein for catheter placement and was excluded for this reason. Another find referred to a congress report from the "3rd World Congress Vascular access" in Berlin in 2014. This article was excluded because it contains only contents for catheter placement in premature and new-borns.
Two publications on the practical application of ultrasound technology for shunt points in dialysis facilities were found by hand in the 2014 edition of the scientific journals "Dialyse aktuell" and "Spektrum der Nephrologie". Another article appeared in "Spektrum der Dialyse & Apherese" in 2016.
A congress report from the EDTNA/ERCA Congress Dresden - 2015 could also be viewed by hand search on the EDTNA/ERCA homepage. Two lectures, one at the IAD 2014 symposium in Weimar and a second at the 2016 dialysis symposium in Erfurt, are the latest findings.
The costs and revenues of the various forms of intervention were determined on the basis of hospital and dialysis billing data. Publications of the Institute for Health and Social Research (IGES), the Institute for Microdata Analysis (IfMDA) and the Federal Association of Statutory Health Insurance Physicians (KBV) from 2013 and 2014 have been used as literature sources for this chapter of the work. Sources for the calculations are the catalogue for the International Classification of Diseases, Germany (ICD-10-GD 2016), the operation and procedure codes (OPS code 2016) for inpatient use and the physicians' fee scale (GOÄ) with the individual evaluation standard (EBM) for billing outpatient medical services. Average personnel costs, both outpatient and inpatient, were determined based on the collective agreement for public service (TVöD) 2016.
For the economic evaluation of the costs of creating a CVC, a shunt, as well as radiological and surgical shunt intervention, the PubMed search revealed 165 articles originating exclusively from the Anglo-American region. Keywords were: vascular access, cost analysis, haemodialysis. 12 articles could be included in the evaluation. A survey from Switzerland was found by hand search in Google Scholar.
PubMed has published 5060 articles evaluating the quality of life of dialysis patients. The search for quality of life in connection with vascular access resulted in a hit rate of 393, none of the articles investigates the direct connection between puncture technique / shunt puncture and quality of life.
In Germany, there are 636 dialysis facilities as main sites and 190 secondary sites (cf. Drabinski, 2014, p. 22). Contact was made with 5 facilities in which the puncture technique is used by doctors and/or nursing staff. Further written inquiries were made to the nephrological professional associations, the nephrological care groups association (fnb) and the working group for nephrological nursing staff (AfnP) as well as the direct approach of lecturers at congresses and conferences. The feedback corresponds to the inquiries in the dialysis facilities.
4. The use of ultrasound-guided shunt cannulation
The following chapter gives an overview of the state of knowledge on the application of ultrasound-guided shunt puncture in dialysis machines at the time of writing this paper. It contains information on investigations from Germany, the Czech Republic, Great Britain, the USA, Canada and Saudi Arabia. All investigations are summarised in Annex 3, Table 12.
The three PubMed research articles were published in the USA, Canada and Japan in 2015 and 2016. The first publication from 2015 is an individual case study from New York by Roshan et al.: "Bedside Ultrasonography for Arteriovenous Fistula Cannulation". In "Seminars in Dialysis", the authors report on the early ultrasound puncture (US puncture) of an AVF in a 77-year-old patient with CVC, increased inflammation parameters, chills/fever and germ detection in blood culture. Puncture problems occurred after removal of the CVC. The vessel was deeper than 1 cm under the skin with a short puncture distance at the same time. As a result, the authors concluded that after the establishment of ultrasound-supported venepuncture and CVC equipment in emergency medicine, this technique is also justified in dialysis therapy for shunt puncture. Especially since US is already being used as standard in dialysis facilities for vascular diagnostics before shunting, for measuring shunt flow and for controlling stenosis (cf. Roshan et al., 2015, p. 433f.).
In 2015, Canadian authors published a training concept for competence development for the use of US technology for shunt puncture. Marticorena et al. describe in "Development of competencies for the use of bedside ultrasound for assessment and cannulation of haemodialysis vascular access" the practical procedure for training qualified nursing staff to work with US on shunt puncture. They point out that the use of ultrasound-assisted shunt puncture in various dialysis centres in Canada and worldwide is standard practice and, in the opinion of the authors, represents the highest quality standard for the puncture of a vascular access. The authors of the training concept emphasize that ultrasonic competence can only be acquired through daily practical application and that approximately 500 punctures are required to master the complex processes (cf. Marticornea et al., 2015, p. 28ff.).
In February 2016 Kamata et al. published a review: "Ultrasound-guided cannulation of haemodialysis access". They are investigating the possibility of ultrasound support for the puncture of various dialysis accesses. They describe the advantages of safe puncture in difficult vascular conditions, the technique of puncture, the two types of vascular imaging for finding the needle tip, the puncture of the AVF and the CVC system. The authors believe that mastering such a complex method requires theoretical knowledge, practical experience and continuous application (cf. Kamata et al., 2016, p. 1ff).
In 2013, Dr. Morgenstern reported on the practical application of ultrasound-guided shunt puncture from his dialysis unit at the Koblenz Protestant Abbey in an issue of "Dialyse aktuell": "Sonographically guided shunt puncture. 8 years of experience with systematic application in a single centre". He describes in detail the method, its advantages for patients and staff, the instruments required and the results for its installation. Through the repeated use of ultrasound technology, employees can gain basic insights into the shunt process, recognize changes at an early stage and initiate pre-emptive measures. In the author's opinion, ultrasound-guided puncture control provides immediate information about the type of puncture error. The author sees further advantages in the planning of the shunt system. With the knowledge that it is also possible to puncture very small-bore and deeper vessels, the surgeon can also consider other, otherwise rather unsuitable vessels for the shunt system. The number of CVC and PTFE prostheses was reduced to 0 - 2 % (GHIA recommendation below 10 %) in Koblenz. Structured training of nephrological nursing staff enables a wide range of applications in everyday work with a high level of acceptance and a relaxed atmosphere for patients and nursing staff. Dr Morgenstern and his team recommend the puncture method for broad application because it improves the quality of dialysis (cf. Morgenstern, 2013, p. 184ff.).
W. Albers from the Klink Bremen published in 2014 an article in the "Spektrum der Nephrologie" on the topic of "Quality assurance and process optimization through ultrasound-assisted puncture in problematic dialysis shunts". The focus of the work is on the appropriate and gentle puncture of the vascular accesses to avoid in-patient stays. According to his data, one third of all hospital admissions of dialysis patients are due to shunt puncture and flow problems. He describes the classification of vascular access with evidence level and the importance of ultrasound-guided imaging for preoperative diagnostics for shunt insertion. For quality assurance of shunt maturation and documentation of sufficient blood flow in the shunt, he sees regular ultrasound checks as mandatory. He sees reasons for an ultrasound-supported puncture in the safe puncture of AVF and PTFE prostheses. Hematomas can be prevented by faulty puncture with effects on the shunt flow, the position, extent and depth of badly palpable vascular prostheses can be determined more reliably and not least the psychological stress of the patients at the time of puncture can be considerably reduced (cf. Albers, 2014, p. 12ff.).
M. Hennrich from Würzburg published in 2016 an article in the "Spektrum der Dialyse & Apherese" entitled: "Relaxed puncture with ultrasound. Why is ultrasound shunt puncture worthwhile?" In this first episode, the series of publications identifies the areas of application, addresses the benefits from the point of view of staff and patients and the cost reduction due to the lower hospitalisation rate. The author of the article assumes a time saving in relation to the consequences of an incorrect puncture (cf. Hennrich, 2016, p. 12).
[...]
- Quote paper
- Angela Drähne (Author), 2017, Ultrasound-guided Cannulation. A Health Economic Consideration, Munich, GRIN Verlag, https://www.grin.com/document/436426

Similar texts








Publish now - it's free

Comments