Excerpt
Contents
I. Introduction
1.1 Pancreatic cancer
1.1.1 PDAC development and progression
1.1.2 Microenvironment
1.1.3 Current treatment options and their limitations
1.2 Oncolytic viruses
1.2.1 Vesicular stomatitis virus
1.3 Signal transducer and activator of transcription 3
1.4 Aim of this thesis
II. Material
2.1 Cell lines
2.2 Reagents
2.3 Antibodies
2.4 Consumables
2.5 Appliances
III. Methods
3.1 Cell culture
3.1.1 3D cell culture systems
3.1.2 Co-culture systems
3.2 Viability assay
3.3 Tissue culture infection dose
3.4 Western blotting
3.5 Flow cytometric analysis
3.6 Confocal microscopy
3.7 Luciferase assay
3.7.1 Plasmid DNA preparation
3.7.2 Transfection
3.7.3 Interferon induction and response
3.8 Scratch assay
IV. Results
4.1 PDAC cells are susceptible to rVSV-GFP-mediated oncolysis in vitro
4.2 S3I-201 causes reduction of PDAC cell viability in vitro
4.3 Combination therapy enhances PDAC killing and safety
4.4 Combinational therapy in the microenvironment
4.5 Effects of S3I-201 and VSV in co-culture
4.6 Combination therapy in 3D
4.7 Inhibition of migration
V. Discussion
VI. List of Abbreviations
VII. References
Abstract
Being the most common malignancy of the pancreas, pancreatic ductal adenocarcinoma (PDAC) displays 5-year survival rates below 6% and ranks among the deadliest types of cancer, especially in the Western world. Several approaches have been explored to improve the outcome of this disease, but the highly complex biology and the aggressive nature of this malignancy require improved and novel therapeutic approaches.
Recently, oncolytic viruses have emerged as an innovative strategy to treat tumors. Exploiting defects in antiviral signaling in tumor cells, oncolytic viruses target and replicate only in cancer cells, while leaving healthy tissues generally unaffected. In particular, vesicular stomatitis virus has proven itself to be an effective oncolytic agent, due to its rapid life cycle and ability to rapidly lyse tumor cells.
In parallel, accumulating evidence has revealed the tumorigenic role of signal transducer and activator of transcription 3 (STAT3). Through its positive regulation of many oncogenic pathways responsible for cancer initiation, progression and metastasis, it has gained increasing interest as a novel therapeutic target. Based on the outcome of previous studies, we hypothesized that a therapy or rVSV-GFP in combination with STAT3 inhibition in vitro would not only lead to an improved anti-tumor response in PDAC cells, but would also improve the safety in healthy tissues. Within the scope of this thesis, two-dimensional, three- dimensional as well as co-cultural in vitro studies were performed, with the aim of characterizing the effect of a combining these two therapeutic agents.Based on our results, we were able to show that both, rVSV-GFP and the STAT3 inhibitor S3I-201, have cytotoxic effects in PDAC cells in vitro. However, a combination therapy resulted in enhanced tumor cell killing in an additive manner, while attenuating viral replication in healthy primary pancreatic cells, being the case in. Further investigations in tumor spheroids revealed that these effects seem to be due to the induction of apoptosis, while the combination of both agents even improved the spread of apoptotic cells through the three-dimensional tissue architecture. In addition, we observed that the combination therapy significantly reduced the migratory and proliferative potential of both, PDACs and cancer- associated fibroblasts.
Substantiated by our results, we believe that combining oncolytic virus with STAT3 inhibitors is a novel treatment option for improving the dismal prospects of PDAC. This approach revealed not only cytotoxic effects on the cancer cells, but due to its anti-proliferative properties and its lytic effect on the stromal cells, it is represents a promising multi-mechanistic therapy for modulating the PDAC microenvironment and potentially resolving the tumor. This work provides preliminary data to support further testing in vivo and the potential future development for clinical translation.
I. Introduction
1.1 Pancreatic cancer
Pancreatic ductal adenocarcinoma, PDAC in short, is the most common malignancy of the pancreas. With a 5-year survival rate of less than 6%, it belongs to the deadliest types of cancer and is the fourth leading cause for cancer related deaths in the United States (Rossi, Rehman et al. 2014). Even though the most survival rates of cancer have been increased in the past few decades, PDAC still displays increasing incidence, especially in the Western world (Xu, Pothula et al. 2014). According to the latest statistics in epidemiology, PDAC is anticipated to become the second most common cause for cancer-related deaths right behind lung cancer in 2022.
The reason for such dismal prognoses is due to the fact that pancreatic ductal adenocarcinoma poses a challenge for both, clinicians and researchers. Already diagnosis of this disease is challenging, since PDAC exhibit symptoms only at very late stages (Kleeff, Korc et al. 2016). Besides owing to a lack of specific markers, there is no molecular approach to identify pancreatic cancer. Also medical treatment is limited as prevalent mutations are not really druggable yet. In addition, this disease exhibits an extremely aggressive nature, which results in rapid high level metastases (Sharma NK 2014). Furthermore, the tumoral environment is particularly relevant for PDAC, since its surrounding highly dense stroma supports cancer progression, while it impedes the accessibility of therapeutics and the immune system (Feig, Gopinathan et al. 2012).
Described above are just few explanations among many others, why PDAC is challenging not just on a molecular level but also in translational research and clinical application. To understand its extremely malignant and multifaceted nature, further insight into the evolution and expansion of pancreatic cancer is necessary.
1.1.1 PDAC development and progression
Besides risk factors as smoking, obesity and aging, also pancreatitis and genetic predisposition concur to the likelihood to develop pancreatic cancer (Klein 2012). Crucial for the development of PDAC are phenotypical as well as genotypical changes, both caused by particular mutations in the genome. The development of PDAC is a complex step by step process, of which each step is initiated by a specific mutation (Bardeesy and DePinho 2002). Once the first mutations appeared, genetic instability in these cells is accumulating, which drives the probability of the acquisition of new mutations in a positive feedback loop manner.
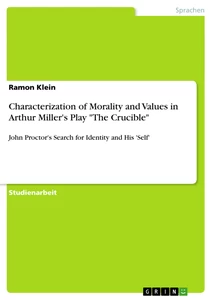
The first step in the emergence of this disease is the dedifferentiation of acinar cells to an embryonic progenitor phenotype in the pancreas. This initiating event is caused by epigenetic silencing of Ptf1a, an acinar cell identity factor, and the upregulation of Pdx1, responsible for pancreatic development and the maturation of β-cells (Pinho, Rooman et al. 2011).
illustration not visible in this excerpt
Figure 1: Different stages of PDAC development are dependent on particular mutations
Cancer development is initiated through acinar to ductal metaplasia, mainly induced by Ptf1a and Pdx1 aberrations. Kras upregulation and EGFR overexpression initiates PanIN formation, which progression through its different states is dependent on further mutations in the genome (i.e. CDKN2A, TP53). Histological pictures were adapted from Brosens et al., 2015
Acinar cell dedifferentiation lays the foundation for the subsequent acinar to ductal metaplasia, ADM in short. If naturally occurring, for example in pancreatitis, this is a reversible mechanism which aids the regeneration of the cell after inflammation or an injury.
Besides Pdx1, SOX9 and Notch signaling are important factors for this transdifferentiation to a ductal-like cell (Storz 2017). But also inflammatory macrophages are capable of initiating this event by cytokine signaling. Hence, also IL-6 induces ADM through the activation of the JAK-STAT3 pathway (Yaqing Zhang and Zetter 2013). Furthermore, ADM can also be irreversible if mutations in Kras occur, which leads to the activation of oncogenic Kras and the initiation of pancreatic intraepithelial neoplasias (PanINs) (Shen, Wang et al. 2013). PanINs represent different progressive stages that need to be passed through for the development of PDAC, which are histologically characterized by morphological alterations compared to the healthy pancreatic duct. Subdivided into three different states, each of them are associated with specific genetic mutations.
As mentioned above, the first stage, PanIN1, is initiated by oncogenic mutations in Kras and its hyperactivation. This induces many pro-proliferative pathways which include but are not limited to the RAF-MEK-ERK and the PI3K-AKT pathway (Ferro and Falasca 2014). Kras activity is also accumulating by the overexpression of EGFR. With the progression of this stage, also the capability of senescence is lost through the loss of CDKN2A. The following loss of TP53, the most prominent and important tumor suppressor gene, is typical for PanIN2 and the first nuclear abnormalities. With the accumulation of genetic instability and the loss of two other tumor suppressor genes, SMAD4 and BRCA2, the neoplastic progression reaches its last state PanIN3, also referred to as carcinoma in situ (Bardeesy and DePinho 2002). At this stage, the neoplasia is histologically hardly distinguishable from pancreatic ductal adenocarcinoma, which is then reached with further aberrations of the genome that enables the tissue of invasiveness and metastasis.
1.1.2 Microenvironment
Besides genetic mutations also PDACs microenvironment plays a crucial role not just for its development but its progression and maintenance as well. A mature pancreatic cancer is histologically defined as tumor islands that are surrounded by its dense stroma. Hence, the desmoplastic regions can account for up to 90% of this disease (Xie and Xie 2015). Being a hallmark of cancer, these regions are highly heterogenous. They consist of cellular components like cancer associated fibroblasts (CAFs), pancreatic stellate cells (PSCs) and immune cells, as well as acellular extracellular matrix (ECM), growth factors and cytokines. All these components form a complex network and the interplay with each other as well as the cancer cells is crucial for cancer initiation and progression (Xu, Zhou et al. 2016).
An important role in these interactions play cancer associated fibroblasts, which are known to promote the progression and metastasis of PDAC. This is achieved by the secretion of growth factors and inflammatory cytokines, the mediation of ECM formation and suppressing the immune system. Vice versa, CAFs are activated by the cancer cells. As a consequence, α-SMA, expressed by activated stromal cells, belongs to negative prognostic markers for PDAC in the clinics (von Ahrens, Bhagat et al. 2017).
As shown in Figure 1, SMAD4 deficiency as well as Kras hyper activation play important roles in PDAC. This is also attributed to the interaction with its stroma. It was shown for this combinational mutation that it leads to an constitutive activation of the TGF-β, resulting in accelerated CAF and PSC proliferation, enhanced ECM production and eventually induced angiogenesis via the VEGF pathway (Ahmed, Bradshaw et al. 2017). Furthermore, the constitutive IL-6 production of the stromal cells over activates the STAT3 pathway in tumor cells in a paracrine manner. This pathway is commonly known for its role in oncogenesis as well as its capability of initiating metastasis via the induction of epithelial to mesenchymal transition (EMT) (Nagathihalli, Castellanos et al. 2016).
Besides many others, aberrational signaling via TGF-β and IL-6/STAT3 are examples to display the importance of the tumor-stroma-interactions within pancreatic ductal adenocarcinoma. As a result, many studies have taken this into account for the development of novel treatment options.
1.1.3 Current treatment options and their limitations
Both, treating PDAC as well as developing new therapeutic options display major challenges to clinicians and researchers. Surgery still remains the most effective option to cure pancreatic cancer completely. In former times, surgical resection was questionable due to high morbidity and mortality rates. Nowadays, however, increased experience led to improved surgery. As a consequence, successfully resected PDACs display 5-year survival rates of up to 20%, which is significantly higher but frankly still not promising (Kleeff, Korc et al. 2016). Additionally, pancreatic cancer barely exhibit symptoms at early stages and specific markers for this disease are non-existent. Given the aggressive nature, this results in advanced stages of PDAC and metastatic spreads throughout the whole body at the time of prognosis (Kamran, Patil et al. 2013). Therefore, surgery is rarely a possible treatment option when PDAC is diagnosed.
Another approach to counteract PDAC is chemotherapy. In the 1950s, 5- Fluorouracil (5-FU) was the mainline chemotherapeutic, resulting in mean survival rates of less than 6 months. This was improved with the finding of gemcitabine mono therapy that extended the survival rates to almost 1 year (Burris, Moore et al. 1997). The most noteworthy approach to optimize chemotherapy was FOLFIRINOX in 2011, a combinational approach consisting of 5-FU, irinotecan, leucovorin and oxaliplatin. Despite to the fact, that it displays significantly increased toxicity, its considerable increased survival benefit made FOLFIRINOX to one of the most widely used chemotherapeutic for advanced metastatic pancreatic cancer (Conroy, Desseigne et al. 2011). The problems with treating PDAC via chemotherapeutics is attributable to many different reasons. First, most of the prevalent mutations illustrated in Figure 1 are hardly druggable yet. This hampers the progress that is achieved by researchers, since the findings are difficult to apply translationally. Additionally, it was shown that PDAC is able to develop resistances to extant therapies, which again decreases the survival chances (Schober, Jesenofsky et al. 2014). Furthermore, PDACs microenvironment mentioned above is crucial for limiting the treatment efficacy. Its abundant stroma embed the tumor cells in a highly dense entity, limiting the vascular perfusion (Khan, Jaggi et al. 2015). As a result, adenomatous components of the tumor are reached in a marginally amount and chemotherapeutics are not able to access their target.
Owing to the many tumor supportive effects exerted, PDACs stroma became a commonly targeted treatment option for many researchers. However, due to contradictory findings it remains unclear if depleting the microenvironment of pancreatic cancer increases the survival. First approaches were conducted by inhibiting sonic hedgehog signaling (Shh), a protein responsible for the paracrine activation of stroma cells, which reduced desmoplasia and increased the survival rates in mice, but clinical trials were stopped because of their poor performance. Further studies for Shh ablation resulted in even more aggressive tumors with increased metastasis (Mei, Du et al. 2016). Other studies have tried to achieve this by the inhibition of matrix metalloproteinases (MMPs) (Zervox, Franz et al. 2000). MMPs are upregulated by cancer cells during EMT and are crucial for the initiation of metastasis. However, inhibiting MMPs resulted in contradictory and partly more aggressive tumors as well. To some extent this was also shown for targeting CAFs (Carr and Fernandez-Zapico 2016). Nevertheless, targeting stroma still eventuated in increased vascularity, which could potentially increase the efficacy of chemotherapeutics. Additionally, due to the tumor suppressive role of PDACs microenvironment, its ablation could possibly lead to an enhanced anti- tumoral activity of the immune system (Xie and Xie 2015). Recent studies have also suggested, that an approached equilibrium could be the solution, which would keep the stroma in rein but does not ablate it (Kota, Hancock et al. 2017).
Considering the many limitations that current treatment options display, the necessity of novel treatment options is obvious. Despite approaches like precision medicine and immunotherapy, oncolytic viruses could be one of those.
1.2 Oncolytic viruses
Oncolytic viruses (OVs) are either genetically modified or naturally occurring viruses that selectively target and replicate solely within tumor cells while not harming the healthy cells of the host (Altomonte and Ebert 2012).
The fact that particular viruses are able to kill cancer cells was recognized already in the early 20th century, when tumors regressed in patients after acquiring a natural infection. Afterwards, various approaches were undertaken to exploit the anti-tumoral effect of viruses. But even if clinical trials led to tumor regression, lack of knowledge in those days resulted mostly in failure of treatment (Hartkopf, Fehm et al. 2012). Nowadays, knowledge increased in immunology and tumor biology, as well as we have the possibility of genetically engineering the genome. Hence, this therapeutic approach gained much interest, especially in the last decade as two genetically engineered OVs have been approved for cancer therapy. In 2005, Oncorine, or H101, an adenoviruses with a deletion in the E1B-gene, was approved in China for the treatment of esophagus and head and neck cancer (Yu and Fang 2007). More recently, T-Vec, a herpes simplex virus that was genetically armed with granulocyte macrophage colony-stimulating factor (GM-CSF), was approved by the FDA in the USA in 2015 and one year later in Europe and Australia for treating melanoma (Kohlhapp, Zloza et al. 2015).
Even though further investigations have to be done for the complete comprehension, OVs are thought to kill cancer cells via two steps. First, they replicate selectively within tumor cells as the have many traits that provide a selective advantage for the virus. Besides hallmarks of cancer like sustained cell proliferation, resisting cell death and avoiding the immune system, the most important abnormality is that tumor cells are defective in their protection mechanisms against viral infection (Kaufman, Kohlhapp et al. 2015). For example, the Interferon (IFN) signaling pathway, which is the very first antiviral response as soon as cells get infected. Additionally, tumor cells can be resistant to signaling of the protein kinase R (PKR), responsible for the detecting and responding to the viral genome (Singh, Doley et al. 2012). Although OVs are also able to infect healthy tissues, they get cleared by the antiviral response, while retaining and further replicating in the neoplastic cells.
As a second step, tumor cells get lysed and release tumor antigens and OVs again. While the virus is then able to distribute further throughout the tumor and infect the cells in a positive feedback loop manner, the released tumor antigen potentially activates a host immune response against the cancer (Jhawar, Thandoni et al. 2017).
OVs exhibit advantages which are missing in many current therapeutic options. They are highly selective for tumor cells while just minimal toxicity was detected for some viruses (Chiocca 2002). Additionally, as the pharmacokinetics of classical therapeutic drugs rather decrease over time, OVs are able to amplify themselves during treatment, resulting in an enhanced anti-tumoral response. Besides, today’s advances in genetic engineering allows the modification of these therapeutic agents, enabling to improve the tumor killing effect and reducing toxicity in healthy tissues at the same time (Goldufsky, Sivendran et al. 2013). Particularly remarkable is the fact, that OV treatment could eventually counteract not just tumors but also metastasis through both active infection of them as well as priming the immune system against tumor antigens (Park and Choi 2016). Lastly, since OVs exploit many different oncogenic features, development of resistances are rather unlikely and weren’t seen so far.
Contrary to the many positive effect of OVs, they also show some disadvantages. Especially delivery of the virus hampers therapeutic efficiency. Intravenous or intraarterial administration of the virus mostly leads to its rapid recognition and destruction via the complement system as well as the innate immune system. Intratumoral injection is hence usually the best option for delivery, but would make the treatment conditional on the tumor site, which is not always accessible for injections (Seymour and Fisher 2016). Furthermore, the tumor microenvironment, which plays a crucial role especially for pancreatic cancer as mentioned above, is another hurdle by limiting OVs ability to spread throughout the whole tumor (Wojton and Kaur 2010). And as these therapeutic agents are indeed quite harmless for healthy tissues, there were still some cases were toxicity was detected, which is still the reason for the failure of some clinical trials.
Nevertheless, OVs belong to the major promising approaches and are considered as breakthrough in immunoncology (Fukuhara, Ino et al. 2016). Within the scope of this thesis, we were working with the Vesicular stomatitis virus (VSV).
1.2.1 Vesicular stomatitis virus
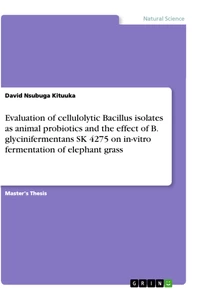
VSV is a bullet shaped virus that belongs to the family of the Rhabdoviridae. Its genome consists of 11 kb single stranded RNA and as depicted in Figure 2, it is encoding for 5 different proteins: the Glyco- (G), Matrix- (M), Large- (L), Phospho- (P) and Nucleoprotein (N).
illustration not visible in this excerpt
Figure 2: Architecture of Vesicular stomatitis virus
The bullet shaped envelope of VSV is covered with Glycoproteins, responsible for the attachment to the host cell. Within the virion, the genomic RNA is tightly encapsidated by the Nucleoproteins. The phosphoprotein together with the Polymerase (encoded by the L-protein) is translating the genome into the mRNA. The Matrixprotein serves the blocking of the hosts cellular response. Picture was adapted from Viralzone (viralzone.expasy.org)
The G-protein allows VSV to entry the host cell via binding LDL receptors on its membrane, which is then uptaken through endocytosis. The N-protein tightly encapsidates the genome of VSV, which is recognized solely by the viral RNA polymerase, encoded by the L-protein, which translates the mRNA together with the P-protein. The purpose of the M-protein is to inhibit cellular responses of the host cell to the infection. This is accomplished by migrating to the nuclear envelope and interacting with Rae1 and Nup98, factors that are necessary for the nucleocytoplasmic trafficking of cellular mRNAs and snRNAs. Natural hosts of VSV include mostly horeses, cattle and pigs. VSV infection in humans are rarely linked with the occurrence of symptoms and are limited to people with direct and frequent contact with this virus (Heiber, Xu et al. 2011).
Contrary to many other OVs, VSV exhibit many natural occurring advantages. To begin with, VSV is a virus model that was already extensively investigated, which alleviates to conceive coherences more quickly. Additionally, it infects the cells mostly independent of their cell cycle, which again facilitates the work with this virus. Since it is a single stranded RNA virus and it replicated within the cytoplasm, there is no risk that the viral genome integrates into the hosts DNA. Another aspect, which is important when trying to establish a virus for oncolytic therapy, is the lack of pre-existing immunity in humans, otherwise it would be immediately recognized by the immune system and eventually hamper the delivery of OVs. Lastly and more importantly, VSVs small genome is easy manipulated, allowing the insertion of oncoselective and oncotoxic factors, as well as the deletion of genes that could potentially harm healthy tissues (Hastie and Grdzelishvili 2012).
Many different approaches have been done to improve VSV. Obviously, a VSV- GFP variant was engineered to facilitated the visibility of VSV under the microscope. Furthermore, neurotoxicity was shown in rodents and also once in humans, which would be a dramatic side effect in the clinic. To counteract this, a VSV-∆M51 variant was genetically modified, resulting in increased safety (Simovic, Walsh et al. 2015). Among many other, there are also variants modulating the immune response, encoding suicide genes or cancer suppressor genes (Fernandez, Porosnicu et al. 2002). Another approach is to combine VSV with drugs that potentially increase its killing effect against the tumor while increasing the viral safety at the same time.
1.3 Signal transducer and activator of transcription 3
The signal transducer and activator of transcription 3 is one of the seven members that belong to the STAT family. As the name already implies, the purpose of these proteins is to transduce a signal from the cell surface to the nucleus, where transcription of various genes becomes activated.
Encoded by chromosome 12, the STAT3 protein consists of seven structural and functional distinct domains. The first one is the NH2-domain that forms homotypic dimers as long as STAT is not phosphorylated and in an inactive state. Directly adjacent to it is the coiled-coil domain, interacting with regulatory proteins. Furthermore, there is the DNA-binding domain, responsible for the localization on the promoter on the genome, as well as the SH2-domain, mediating dimerization when activated. These two domains are linked by the linker domain, hence leading to a proper conformation of the protein. Crucial for the activation of the STAT3 protein is the tyrosine activation domain, containing a conserved tyrosine residue which can be phosphorylated at position 705. Lastly, the activation of downstream pathways is then induced by the transactivation domain through the interaction with transcriptional regulators (Darnell 1997).
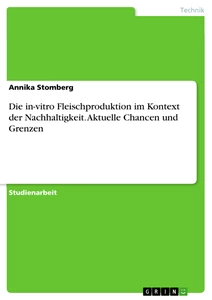
illustration not visible in this excerpt
Figure 3: Activation of STAT3 results in transcription of oncogenic proteins
Once the appropriate receptors are activated by various ligands, a phosphorylation cascade leads to the activation of STAT3. The phosphorylated STAT3 then dimerizes, translocated to the nucleus and acts as transcriptional factor. In that way, many oncogenic genes become activated, resulting in e.g. enhanced proliferation, survival, angiogenesis and invasive potential.
illustration not visible in this excerpt
Figure 3 illustrates the mechanism of action by which STAT3 becomes activated. This can be induced by various cytokines and growth factors like IL-6 or EGF. The receptors responding to such ligands are usually tyrosine kinases, often associated with Janus activated kinases (JAKs). After binding of the ligand, its receptors dimerize and lead to the phosphorylation of JAKs. Subsequently, adjacent tyrosines on the receptor become phosphorylated, which are then bound by the SH2-domain of STAT3 proteins. Once two STAT3 monomers are activated by the phosphorylation at tyrosine 705 (Y705), dimerization and translocation into the nucleus follows. STAT3 acts as transcription factor on the DNA and induces transcription of many downstream effectors that possess oncogenic potential (Yue and Turkson 2009).
STAT3’s tumorigenic role is multifaceted and occurs at all different levels of cancerogenesis, beginning from the induction of cancer, over its progression, up to metastasis. Besides its role in malignant cell transformation, STAT3 is crucial for increased proliferation through upregulation of cMyc and Cyclin D1 (Xiong, Yang et al. 2014). Additionally, it prevents apoptosis by inducing the transcription of Bcl-2 plus negatively regulating p53 (Niu, Wright et al. 2005). Furthermore, STAT3 is essential for migration, invasion, intravasation and angiogenesis, mechanisms that are all determining for metastasizing. Nevertheless, especially remarkable for pancreatic cancer is its function for the paracrine communication with the tumor microenvironment (Nagathihalli, Castellanos et al. 2016). It was shown that STAT3 activates fibroblasts and enhances their proliferation through the TGFβ pathway, resulting in fibrotic reactions. At the same time, CAFs secrete high amounts of IL-6, one of the most important cytokine for the activation of STAT3, which results in a positive feedback loop (Zhu, Zhang et al. 2014).
Although inactivating STAT3 leads to embryonic lethality in mice, it was shown that its role in healthy adult tissue is unimportant (Kamran, Patil et al. 2013). Hence, given the high oncogenic potential of STAT3, its inhibition gained increasing interest for translational application in the clinic. As a consequence, the inhibitory capability of both naturally occurring substances and synthetically derived chemical agents were investigated. Within the scope of this thesis, we were working with the chemical probe inhibitor S3I-201, also called NSC 74859.
illustration not visible in this excerpt
Figure 4: Chemical structure of S3I-201 S3I-201, or NSC 74859, prevents dimerization of activated STAT3 monomers by docking to the SH2- domain
The inhibitor depicted in Figure 4 above targets the critical step which leads to the dimerization complex of two activated STAT3 proteins. By docking directly to the SH2-domain, nuclear translocation and hence, transcriptional activation can not happen anymore. It was already shown for S3I-201 that it acts antiproliferative and proapoptotic on malignants cells while being harmless to healthy cells. Furthermore, it was even shown that it can effect tumor regression in xenograft models (Siddiquee, Zhang et al. 2007).
[...]
- Quote paper
- Simon Dedic (Author), 2017, In vitro characterization of oncolytic virus in combination with STAT3 inhibition for improved therapy against pancreatic ductal adenocarcinoma, Munich, GRIN Verlag, https://www.grin.com/document/420553
Similar texts









Publish now - it's free

Comments