Excerpt
Table of Contents
0. Tables and Figures
1. List of Abbreviations
2. Introduction
2.1 Human Malaria
2.1.1 Causative Parasites and their Life Cycle
2.1.2 Clinical Signs and Symptoms
2.1.2.1 General Clinical Features
2.1.2.2 Severe Falciparum Malaria
2.1.3 Diagnosis
2.1.4 Laboratory Findings
2.2 History
2.2.1 History of the Human Malaria Parasites
2.2.2 Geographical Malaria History
2.2.3 History of Malaria Handling
2.3 Epidemiology
2.3.1 Malaria Transmission
2.3.2 Prevalence and Incidence
2.3.3 Endemicity
2.3.3.1 Stable Endemic Malaria
2.3.3.2 Unstable and Epidemic Malaria
2.3.4 Epidemic preparedness, prediction and prevention of epidemics
2.3.5 Epidemiological information systems
2.3.6 Resistance Pattern
2.3.7 Travelers
2.4 Malaria in the Pediatric Population and Pregnant Women
2.4.1 Pediatric Population
2.4.2 Pregnant Women
2.5 Malaria as a Disease of the Poor
3. Global Malaria Control Strategies
3.1 Preventive Measures
3.1.1 History of the Global Malaria Control Strategies
3.1.2 General preventative Measures
3.1.3 Vector Control
3.1.3.1 Insect repellents
3.1.3.2 Insecticide treated nets (ITNs)
3.1.3.3 Indoor Residual Spraying
3.1.3.4 Recommendations
3.1.4 Chemo-Prophylaxis
3.1.5 Vaccination
3.1.6 Other Preventive Measures
3.2 Current Treatment Approaches
3.2.1 Benefits and Liabilities of Existing Anti-Malarial Drugs
3.2.1.1 Quinolines
3.2.1.2 Artemisinins
3.2.1.3 Antifolates
3.2.1.4 Antibiotics
3.2.2 Combination Therapy
3.3 Treatment Policies and practices
3.4 Malaria Prevention and Treatment in Pregnant Women
4. Global Public Initiatives – Public Private Partnerships
4.1 World Health Organization (WHO)
4.1.1 WHO Interactions with NGOs
4.1.2 WHO Essential Drugs
4.1.3 WHO and the Private Sector / Public Private Partnerships (PPPs)
4.2 Special Program for Research and Training in Tropical Diseases (TDR)
4.3 Medicines for Malaria Venture (MMV)
4.4 Roll Back Malaria (RBM)
4.5 Global Alliance for Vaccines and Immunization (GAVI)
4.6 Program for Appropriate Technology in Health (PATH) and Malaria Vaccine Initiative (MVI)
4.7 World Bank
4.8 Bill & Melinda Gates Foundation as an Example for Private Foundations
4.9 Donation-Distribution Partnerships
5. Health Economy
5.1 Malaria associated Economic Measures
5.2 Costs of Anti-Malarial Drugs
5.3 Financing of Anti-Malarial Drugs
5.4 Regulatory Agencies’ Contributions
5.4.1 Orphan Drugs
5.4.2. Pediatric Laws
5.4.3 International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH)
5.5 Pharmaceutical Industry
5.5.1 Overview on Development of New Drugs
5.5.2 Development of New Anti-malarial Drugs
5.5.3 Glaxo Smith Kline (GSK)
6. Discussion
6.1 The Challenge of Malaria in Endemic Countries
6.2 Role of the Endemic Countries
6.3 Public-Private Partnerships (PPPs)
7. Conclusion
8. References
9. Curriculum Vitae
0. Tables and Figures
Tables
Table 1: Characteristics of Plasmodium species infecting humans (Source: [118])
Table 2: Signs and Symptoms of severe malaria in adults and children (Source: [58])
Table 3: Deaths attributable to infectious diseases by region, 2001 (Source:[89])
Table 4: Overview on drugs developed by TDR in cooperation with an industrial partner (source: [94])
Table 5: Philantropic Drug Donation Programmes (Source: [57])
Table 6: The Malarone Donation Programme (Source: http://www.malaronedonation.org)
Table 7: Manufacturer and Current Prices for Artesunate (600mg) and Artesunate plus Amodiaquine Blister Presentations (Source: [29])
Table 8: Committee for orphan medicinal products (COMP) Public Summary of negative opinion for the Orphan Drug Designation of Lapdap (Source: Document EMEA/COMP/1073/02 Rev 1. London 8 January 2003)
Table 9: Attrition rates for the different phases of drug research and development (Source: [75])
Figures
Figure 1: Life cycle P. Falciparum (Source: [2])
Figure 2: Parasite life cycle and pathogenesis of falciparum malaria. (Source: National Center for Diseasae Control, [http://www.cdc.gov/malaria/biology/life_cycle.htm])
Figure 3: Species Identification of malaria parasites in Giemsa stained thick blood films (source: [58])
Figure 4: Appearance of P. falciparum parasite stages in Giemsa-stained thin and thick blood films (source: [58])
Figure 5: Global Distribution of Malaria (Source: [99])
Figure 6: Morbidity and Mortality in Different settings of endemicity (Source: [46])
Figure 7: Global malaria status (source: [120])
Figure 8: Drug-resistant malaria and pesticide-resistant mosquitos (source: [120])
Figure 9: Timing of IPT. (Source: [114])
Figure 10: Overview of malaria co-ordination and funding organisations (Source: [112])
Figure 11: TDR’s Collaborations with the Pharmaceutical Industry (source:[http://www.who.int/tdr/index.html])
Figure 12: TDR Budget by disease, 1999-2000 (source:[http://www.who.int/tdr/index.html])
Figure 13: TDR Budget by research area, 1999-2000 (source: [http://www.who.int/tdr/index.html])
Figure 14: Grants paid by the Bill & Melinda Gates Foundation (Source: http://www.gatesfoundation.org/default.htm)
Figure 15: Per Capita government expenditure on health in Africa (Source: [1])
Figure 16: Overview on development of new drugs (Source: [63])
Figure 17: Industry Costs and Revenues associated with product development (source: [92])
Figure 18: World pharmaceutical market, 1997 (Source: http://www.ims-global.com/insight/report/global/report.htm)
1. List of Abbreviations
illustration not visible in this excerpt
2. Introduction
Malaria is a life-threatening parasitic disease transmitted by mosquitoes. It was once thought that the disease came from fetid marshes, hence the name ‘mal aria,’ (bad air). In 1880, scientists discovered the real cause of malaria—a one-cell parasite called plasmodium. Later they discovered that the parasite is transmitted from person to person through the bite of a female Anopheles mosquito, which requires blood to nurture her eggs[84].
Malaria was eliminated from the United States and from most of Europe during the first half of the twentieth century as a result of changes in land use, agricultural practices, house construction and some targeted vector control. The development of the highly effective, residual insecticide Dichloro-Diphenyl-Trichlorethane (DDT) initiated a global eradicationprogramin the 1950s and 1960s which wasvery successful in many countries such as India, Sri Lanka and the former Soviet Union. However, this success was not sustained because of the costs of theprogram, the resistance of many communities to repeated spraying of their houses and the emergence of resistance to DDT. Furthermore, with the exception of a few pilot schemes, no sustained effort was made to control malaria in sub-Saharan Africa, the main area of malaria endemicity in the world. The elimination of malaria from most of Europe and from North America and the failure of the global malaria eradicationprogramled to a loss of interest in malaria for a period of about 25 years from the early 1970s to the late 1990s. Only 3 of 1,223 new drugs developed during the period 1975–1996 wereanti-malarials [113]. Industry lost interest in the development of insecticides for public health use and support for research on malaria declined. Furthermore, in many malaria-endemic countries, national malaria controlprograms, established during the colonial period and sustained during the period when elimination of malaria was considered to be an achievable goal, collapsed. Thus, for many years, there was little change in mortality and morbidity from malaria, especially in Africa. Recently, the malaria situation has deteriorated and mortality from malaria isincreasing in sub-Saharan Africa [37].
The past five years haveseen a pronounced re-awakening of interest in malaria in the richer countries of the world. Statements on the need for greater efforts to control malaria have been made at a number of high-profilepolitical meetings in Africa and in industrialized countries. Research scientists have had an important catalytic role in this process. In 1997, a meeting was held in Dakar, Senegal, attended by most of the small number of scientists undertaking malaria research in Africa and by their sponsors, which established priorities for a multidisciplinaryprogramof research.[37].
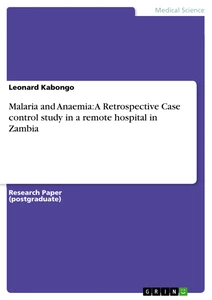
At present, about 100 countries or territories in the world are considered malarious, almost half of which are in Africa, south of the Sahara. Although this number is considerably less than it was in the mid-1950s (140 countries or territories), more than 2,400 million of the world’s population are still at risk. The incidence of malaria worldwide is estimated to be 300–500 million clinical cases each year, with about 90% of these occurring in Africa — mostly caused by P.falciparum andsecondlyby P. vivax. The most important reason for the persistence of malaria in Africa is the presence of the vector Anopheles(A.)gambiae.A. gambiae feeds preferentially on humans and is long-lived, making it particularly effective at transmitting malaria from one person to the next. The entomological inoculation rate (EIR), a measure of the frequency with which an individual is bitten by an infectious mosquito, rarely exceeds 5 per year in Asia or South America. In contrast, EIRs of over 1,000 have been recorded in several parts of sub-Saharan Africa(“Hyperendemicity”). In savannah areas of West Africa, it is not unusual to collect in one room during the course of a single night several hundred mosquitoes of the A.gambiae complex, 1–5% of which are infectious. The task of interrupting transmission in such a situation is daunting [37]. Malariais thought to kill between 1.1 and 2.7 million people worldwide each year, of whom about 1 million are children under the age of 5 years in Africa. These childhood deaths, resulting mainly from cerebral malaria and anemia, constitute nearly 25% of child mortality in Africa and take more than 2000 young lives every day in the world [1], [37], [99]. or one life every 30 seconds.Case fatality rates of 10–30% have been reported among children referred to hospital with severe malaria, although these rates are even higher in rural and remote areas where patients have restricted access to adequate treatment [94]. In endemic countries, one third of all clinic visits and at least a quarter of all hospital admissions are for malaria [1].
One of the biggest achievements in Public Health is the development of vaccines for polio and other diseases which has been fundedpublicly [56], and malaria should follow these examples .
Deaths from malaria in countries outside Africa occur principally in non-immune people who become infected with P.falciparum in areas where diagnosis and treatment are not available. One of the greatest challenges facing malaria control worldwide is the spread and intensification of parasite resistance toanti-malarialdrugs. The limited number of such drugs has led to increasing difficulties in the development ofanti-malarialdrug policies and adequate disease management. The challenging task is to overcome resistance and develop safe and effective drugs as well as sustainable preventive measures mainly in young children and pregnant women [94].As the disease mainly occurs in the poorest populations of the world the pharmaceutical industry in developed countries has little economic interest in the development of anti-malarial drugs (littl e chance of profits or only break-even point for investment). Therefore, a system of incentives has to be established in order to make drug development in this sector more attractive to the innovative pharmaceutical companies.
2.1 Human Malaria
2.1.1 Causative Parasites and their Life Cycle
Malaria is a protozoan disease transmitted by the bite of Anopheles mosquitoes. It is the most important parasitic disease in humans. Four species of the genus Plasmodium infect humans:
-P.falciparum
- P. malariae
-P. vivax
- P. ovale.
Recently, a fifth species has been found to be causative for human malaria: P. knowlesi which was previously thought to be infective inlong-tailed macaquemonkeys only. Obviously, P. knowlesi infections have been wrongly diagnosed as P.malariae malaria.Further work is needed to determine whether human P. knowlesi infections are acquired from macaque monkeys or whether a host switch to human beings has occured [107].
Among the four well-known species of human malaria, P.falciparum stands out as the most malignant form and the only one where severe complications such as cerebral malaria, severe anemia, renal failure and pulmonary affection are frequently seen.Somefeatures , important for disease severity and pathogenesis, separate P.falciparum from the other human malarias: the ability to invade erythrocytes of all ages causing very high parasitemias,enhanced growth and the capacity to adhere to vascular en d othelium through the process of sequestra tion. The infected erythrocyte can adhere to the endothelium and to uninfected erythrocytes via parasite-derived proteins expressed on the surface of the infected erythrocyte. This enables the parasite to avoid clearance by the immune system in the spleen. The adherence causes a considerable obstruction to tissue perfusion. The destruction of the red blood cells is an inevitable part of falciparum malaria[42],[64].
Genetic differences between individuals regarding the immune response mounted by the host are also of great significance for bringing about severe disease. Many hypotheses have been formulated to explain the pathology behind severe falciparum malaria, no final mechanistic explanation has yet been found[42].
Infection with P. vivax and P. ovale, can cause disease relapse as parasites can rest in the liver for several months up to four years after a person is bitten by a mosquito [112], [118].
illustration not visible in this excerpt
Table 1: Characteristics of Plasmodium species infecting humans (Source:[118])
Human infection begins when a female anopheline mosquito , the disease vector, inoculates sporozoites from its salivatory glands during a blood meal. A vector in general is an animal that transmits a pathogen, or something that causes a disease, to another animal. Mosquitoes are the only vectors for malaria, but only 60 out of the 380 species of anopheline mosquitoes can host malaria-causing plasmodium. Three-fifths of the female a nopholes mosquitoes, like their sisters of other lines, are dependent on blood meals to feed their maturing eggs. While sipping blood, a plasmodium -infected female mosquito injects thread-shaped, infectious agents called sporozoites into her human host. Sporozoites circulate for a time (less than 5 minutes) and then enter the parenchymal cells of the liver to hide out from the immune system (intrahepatic or pre-erythrocytic merogony) . Here, they live for one to two weeks, multiplying asexually to produce thousands of offspring . The swollen liver cell bursts, discharging invasive merozoites into the bloodstream an event that initiates the symptomatic stage of the infection. In P. vivax and P. ovale infections , a proportion of the intrahepatic forms do not divide immediately but remain dormant for months before reproduction starts. These “sleeping forms” or hypnozoites are the cause of the relapses that characteri z e infection with these two species. Later, hypnozoites mature to reinvade other liver cells, where they continue to produce more merozoites, causing recurring bouts with malaria. Interestingly, the most deadly species, P .falciparum, does not produce these hypnozoites. Merozoites enter red blood cells to feed on the blood. They reproduce asexually to form more merozoites, which invade other red blood cells. This cycle continues unless stopped by the body’s defenses or medicine. While in the red blood cells, some merozoites mature into male and female gametocytes that are long-lived and not associated with illness . Upon release, these do not enter the red blood cells, but circulate awaiting transfer to the mosquito host. The female mosquito takes her blood meal and simultaneously sucks up some of the gametocytes. In the mosquito’s stomach, the male gametocyte (sperm) and the female gametocyte (egg) fuse and form a zygote . This stage matures to form an ookinete, which penetrates and encysts in the mosquito ’s gut wall. The resulting oocyst expands by asexual division until it bursts to liberate thousands of sporozoites. The sporozoites migrate to the salivary glands of the mosquito for their journey into a human host. The disease in humans is attributable to the direct effects of red cell invasion and destruction a nd the host’s reaction to this process[2].Figure 1 diagrams the life cycle Plasmodium falciparum [2].
illustration not visible in this excerpt
Figure 1 : Life cycle P. Falciparum ( Source:[2] )
illustration not visible in this excerpt
Figure 2 : Parasite life cycle and pathogenesis of falciparum malaria.(Source: National Center for Diseasae Control, [http://www.cdc.gov/malaria/biology/life_cycle.htm])
The malaria parasite life cycle involves two hosts. During a blood meal, a malaria-infected female Anopheles mosquito inoculates sporozoites into the human host . Sporozoites infect liver cells and mature into schizonts , which rupture and release merozoites . (Of note, in P. vivax and P. ovale a dormant stage [hypnozoites] can persist in the liver and cause relapses by invading the bloodstream weeks, or even years later.) After this initial replication in the liver (exo-erythrocytic schizogony ), the parasites undergo asexual multiplication in the erythrocytes (erythrocytic schizogony ). Merozoites infect red blood cells . The ring stage trophozoites mature into schizonts, which rupture releasing merozoites . Some parasites differentiate into sexual erythrocytic stages (gametocytes) . Blood stage parasites are responsible for the clinical manifestations of the disease. The gametocytes, male (microgametocytes) and female (macrogametocytes), are ingested by an Anopheles mosquito during a blood meal . The parasites’ multiplication in the mosquito is known as the sporogonic cycle . While in the mosquito's stomach, the microgametes penetrate the macrogametes generating zygotes . The zygotes in turn become motile and elongated (ookinetes) which invade the midgut wall of the mosquito where they develop into oocysts . The oocysts grow, rupture, and release sporozoites , which make their way to the mosquito's salivary glands. Inoculation of the sporozoites into a new human host perpetuates the malaria life cycle.
2.1.2 Clinical Signs and Symptoms
2.1.2.1 General Clinical Features
Malaria begins as a flu-like illness with non-specific symptomssuch asmalaise, headache, fatigue, abdominal discomfort and muscle aches 8-30 days after infection. Typical cycles of fever, shaking chills and drenching sweats may then develop. As the untreated infection becomes synchronised the fever becomes periodic with pyrexial spikes every one or three days associated with chills or rigors. Synchroni z ation occurs earlier with P. vivax and P. ovale than with P. falciparum (coincid ence with parasite multiplication and destruction of red blood cells [RBC] ) . The untreated infection continues for weeks or months in the non-immune patients, but only P. falciparum produces fulminant disease in untreated patients . The classic malarial paroxysms in which fever spikes, chills and rigors (tremors induced by chills) occur at regular intervals are rare. The rigors are more common with P. vivax and P. ovale than with P. falciparum. More often, the fever is irregular at first ; in non-immune adults or children nausea, vomiting and orthostatic hypotension are common. Most patients with uncomplicated acute infections have few abnormal physical findings other than mild anemia and in some cases a palpable spleen[118],[119].
2.1.2.2 Severe Falciparum Malaria
Severe falciparum malaria isdefined by the presence of asexual blood stage parasites in the blood plus one or more of a list of clinical features including neurological impairment, pronounce d anemia, hypogl ycem i a, acidosis, hyperlactatemia, circulatory collapse, multi-organ failure and coag u lopathies[42].
Severe malaria can mimic many other diseases that are also common in malarious countries. The most important of these are all types of meningitis, typhoid fever and septicemia. Other differential diagnoses include influenza, dengue and other arbovirus infections, hepatitis, leptospirosis, the relapsing fevers, haemor r hagic fevers, scrub typhus, all types of viral encephalitis (including rabies), gastroenteritis and, in Africa, trypanosomiasis. In pregnant women, malaria must be distinguished from sepsis arising in the uterus, urinary tract or breast. In children, convulsions due to malaria must be differentiated from febrile convulsions. In the latter, coma usually does not last for more than half an hour, although some children do not regain full consciousness until 30–60 minutes after the ictal phase[58].
Severe malaria is a disorder that affects several organs although the most marked manifestations may seem to involve a single organ such as the brain[64].
Coma is a characteristic feature of severe cerebral falciparum malaria and despite treatment associated with a mortality of approximately 20% in adults and 15% in children. The onset of coma may be gradual or sudden following a convulsion. Approximate l y 15% of patients have retinal hemorrhages. Anemia and jaundice are common. Generalized convulsions are common in children with cerebral malaria and in about half of adults. Seizures are associated with high temperatures. Approximately 10% of children who survive cerebral malaria particul arly those with hypoglycemia , severe anemia, repeated seizures and deep coma have persistent neurologic deficits. Residual deficits are rare in adults[118].In many pediatric patients with cerebral malaria coma seems to be a response to overwhelming metabolic stress rather than a primary problem in the brain. Such children are often profoundly acidotic and may regain consciousness remarkably quickly after appropriate resuscitation, suggesting that cerebral malaria in this instance can not be a consequence of the classical histologi c al picture[64].
Hypoglycemia is associated with a poor prognosis. It has been reported to be of major prognostic significance in malaria-infected children in Malawi and the most serious complication of childhood falciparum malaria in The Gambia predicting the highest mortality of all categories in a group of 604 patients . Children and pregnant women are at special risk. Hypoglycemia results from failure of hepatic gluconeogenesis and increased consumption of glucose by the host and the parasites[18], [118].
Anaerobic glycolysis occurs in tissues where sequestered parasitized erythrocytes interfere with microcirculatory flow. This phenomenon, together with hypotension and a failu re of hepatic lactate clearance causes lactic acidosis. Hyperventilation is the consequence, prognosis is poor[118].
Adult respiratory distress syndrome (ARDS) may develop in adults with severe falciparum malaria even after several days of anti-malarial treatment and clearance of parasites. The pathogenesis is unclear, the mortality rate over 80%[118].
Renal impairment is common among adults with severe falciparum malaria but rare among children. Renal failure is associated with high mortality , the p athogenesis is unclear[118].
Anemia is caused by direct destruction of the erythrocyte s when the parasites (merozoites) are released, by accelerated destruction and removal of red cells by the spleen and by suppression of the bone marrow with ineffective erythropoiesis. Anemia can develop rapidly and transfusion is often required. Anemia is a particular problem in children. In some patients with P. falciparum malaria massive hemolysis causes h emoglobinemia, black urine and renal failure (blackwater fever)[118].
2.1.3 Diagnosis
The diagnosis of malaria rests on the demonstration of the asexual forms of the parasite in peripheral blood films stained preferably with Giemsa. Both, thin and thick blood smears should be made with great care on clean slides. In thin smear, t he level of parasitemia is expressed as the number of parasitized erythrocytes per 1000 red bloods cells and this figure is converted to the number per microliter of blood. Interpretation of thick film results (based on evaluation of white blood cells) is more difficult and requires a lot of experience[118].Nevertheless, thick films are more useful than thin films in the detection of a low-density malaria parasitaemia. Facilities and equipment for microscopic examination of blood films can be easily set up in the side-room of a clinic or ward, and films can be read by trained personnel on site. This reduces the delay that commonly occurs when samples must be sent to a distant laboratory[58].
The relation between the level of parasitemia and the prognosis is complex; patients with excess of 105 per microliter are more likely to die. However, nonimmune patients may die with relatively low parasite densities, and partially immune persons may tolerate relatively high levels with minor symptoms[118].
illustration not visible in this excerpt
Figure 3: Species Identification of malaria parasites in Giemsa stained thick blood films (source: [58])
illustration not visible in this excerpt
illustration not visible in this excerpt
Figure 4: Appearance of P. falciparum parasite stages in Giemsa-stained thin and thick blood films (source: [58])
2.1.4 Laboratory Findings
Normochromic, normocytic anemia is the rule. The leukocyte count is low to normal. The platelet count is usually moderately reduced (to about 100.000 per microliter). In severe infections, the prothrombin and partial prothrombin times may be prolonged and thrombocytopenia may be severe. In severe falciparum malaria, metabolic acidosis may be present with low plasma concentrations of glucose, sodium, bicarbonate, calcium, phosphate, albumin ; elevated plasma levels of lactate, blood urea nitrogen, creatinine, urate, muscle and liver enzymes and conjugated and unconjugated bilirubin. Hypergammaglobulinemia is usual in immune and semi-immune patients. In cerebral malaria, the white blood count often varies between 9000 and 11000 per mi croliter but can be higher than 20000 per microliter, the differential count is usually no rmal[118].
2.2 History
2.2.1 History of the Human Malaria Parasites
P. malariae is a natural parasite of African great apes and humans in Africa. It is found in no other Old World primate species within or outside Africa. As a parasite of the ancestor of both humans and African great apes, ancestral P. malariae would have continued to parasitise and cross-infect both host lineages as they diverged around five million years ago. P. malariae survivesunder tropical and temperate transmission conditions and is adopted to endemicity in sparse and mobile human populations [16].
P. ovale is a strictly warm-climate parasite. Today it is found commonly throughout tropical Africa and in very limited distribution elsewhere in the tropics [16].
P.falciparum and P. vivax each have a close biological relative which is a parasite of African great apes, an argument that speaks in favour of the African origins of both species [16].
Outside Africa, the female mosquito vectors of malaria are zoophilic rather than anthropophilic. In the endemic areas of Africa, 80% to 100% of the vector bites are anthropophilic. This is the most important factor for the stability and the intensity of malaria transmission in Africa today [16].
2.2.2GeographicalMalaria History
Malaria seems to have been known in China for almost 5000 years and in Northern India for 3500 years. Sumerian and Egyptian texts date from 3000 to 4000 years ago. In 323 B.C. beyond Mesopotamia Alexander the Great is said to have died of malaria. Malaria seemsnotto have reached Italy until the second century B.C. By the beginning of the Christian era, malaria was wide-spread around the shores of the Mediterranean, central and south-east Asia, China, Korea, Japan. In the Middle Ages, malaria began to spread in northern Europe[16].
From mid-19th century onward malaria disappeared from Europe mainly due to cheap and widespread availability of quinine although at the beginning of the 20th century large areas of Europe and Northern America werestillaffected (e.g. Mediterranean and Balkan countries, England, Netherlands, much of central Europe and southern Russia ) . By the early 1950s malaria had largely disappeared from North America and almost all of Europe[16],[106].
In Central America and the Caribbean successful vector control via DDT was performed. In South America, malaria was observed only locally, but the situation became complicated due to the resistance of the parasites (mainly P. falciparum) to chloroquine (CQ) .
In Asia, many successful campaigns against malaria were performed due to the high burden of illness (mainly DDT for vector control)[16].
From a European perspective, malaria has long been a formidable problem for the colonizing powers in their dependencies in the tropics, but in times of war the disease has assumed overwhelming importance. In the first world war, malaria was a major problem in several regions of Europe including the Balkans and troops had to be persuaded to take appropriate prophylactic measures. In the second world war, the principal impact was felt in the Far Eastern theatre particularly in the jungles of South-East Asia as well as in malarious areas of Europe and North Africa [21]. By the time of the Korean war 1950-1953, malaria had assumed less military importance. This is partly because the prevalent form of malaria in the Korean peninsula is the incapacitating, but usually not-lethal P. vivax, but also because new potent prophylactic agents had become available. During the American involvement in Vietnam (1964 –1973) malaria forced itself back on the agenda partly due to the incidence of malaria among American forces (390,000 sick days lost to malaria) but also due to the emergence of P. falciparum strains that were resistant to available drugs [38].
2.2.3 History of Malaria Handling
As early as in the sixth century B.C.: the Greeks and the Romans were aware of the association between fever and warm-wet climate as well as stagnant waters and swamps [36], [69]. This awareness led to the drainage interventions aimed at improving the health of the nearby population and increasing agricultural production [36]. Later, other communities throughout much of Europe took up deliberate drainage activities focussing on improvements in public health. Not so long ago, malaria was a summer-time risk in Denmark [69]. With the discovery of the role of mosquitoes as the vector of malaria in India in 1897 first specific interventions to control malaria were introduced. Some of the major environmental-management interventions come from the construction of the Panama Canal and the drying of the Pontine marshes in Italy where land filling and drainage played an important role. In the second half of the 20th century, chemical-based vector control became the dominating strategy (e.g. DDT), and engineering-based interventions like draining, one of the oldest and best documented methods, lost their importance. The renewed interest in environmental-management approaches for the control of malaria is mainly due to
- The rapid development of resistance to the insecticides by mosquitoes
- The increasing cost of developing new chemicals
- Logistic constraints involved in the operation of chemical-vector programs.
In terms of curative treatment, quinine has been used for malaria prophylaxis and therapy for more than 350 years [12], and up to the first world war it had no serious rivals. Since malaria could be treated successfully with quinine and the drug was easily available from the bark of the Chinchona tree there was little pressure for the development of alternatives. During the first world war acute shortage of quinine occured since most of the world’s supply came from Dutch and British plantations in the East. Germany found itself cut off from the world supply of quinine and developed synthetic drugs the first being plasmoquine (later called pamaquine). In retrospect, plasmoquine was hardly a major breakthrough as it proved to be much less effective against human malaria (especially P. falciparum) and turned out to be more toxic than had been hoped. One advantage is that it killed malaria gametocytes and prevented relapse in P. vivax malaria [38].
In recent strategies, the WHO has advocated the use of a multitude of interventions in the control of malaria environmental control measures as well as chemically-based vector control as well as drugs to treat malaria. Some disagreement between the engineering side focusing on preventive measures and the curative medicallytrained professionals over resource prioritization existed in the 20th century. It is evident that the interventions are of a site-specific nature. Without detailed ecological knowledge of the local vector and the epidemiology of the disease any intervention will be a shot in the dark or may potentially do more harm than good [51]. These efforts however led to a decrease of malaria prevalence: today it is 1/10 or less of what it used to be at its height. For case fatality the same figure holds true. With the main exceptions of Europe and North Americaup to subtropical countries, elsewhere in the world, mainly in the tropical regions,the mid-20th century goal of malaria eradication was never realized. The achievement was an unprecedented reduction in morbidity and mortality [16].After malaria had been eradicated in the above mentioned regions, it became almost wholly a disease of the tropics, particularly in Africa[102].T
he malaria problems in Africa were and are of a different type from those confronted anywhere else as the stability and intensity of malaria transmission presenthuge problems. National malaria control organizations were operational in many African countries by the 1950s. The WHO goal of “malaria eradication” failed in Africaand has been abandoned[16] as it
became evident that global eradication was not feasible(particularly due to the vector resistance to DDT and the parasite resistance to CQ and other low-cost first-line drugs[102]).Today the “malaria control programs” are state of the art [16].
Other reasons for abandoning the campaign may have been geopolitical and based on the fact that malaria control had been achieved in the southern USA, southern Europe, southern regions of the Soviet Union, much of Latin America and large parts of Asia. In mid 1970s, the USA had withdrawn from Vietnam so that the US military evinced a sharply reduced concern for malaria control. The major pharmaceutical companies neglected malaria drug discovery or vaccine research because the travelers’ market was small and still handled by existing medicines. Impoverished African countries were not on the geopolitical radar screen[102].
In 1979 a WHO definition made clear that the control of the vectors must not have “adverse effects on the quality of human environment”. Early permanentmodificationsof the environment would have been categorized today asinfluencingecosystems such as wetlands or mangrove swamps. In the early 20th century, the implications for the natural environment were never given much attention. Emphasis was on costing of interventions (direct costs of malaria as well as the wider economic cost of the malaria burden to production systems or society features). Many of the environment interventions could be designed to have additional economic benefits over and above disease reduction as the experimentation with alternate wet and dry irrigation in rice cultivation[115]and the secondary benefit of drainage activities resulting from land reclamation or increased agricultural productivity[39]have shown[51].
2.3 Epidemiology
2.3.1 Malaria Transmission
The malaria burden is not evenly distributed. The global pattern of malarial transmission suggests a disease cent e red in the tropics, but with a reach into subtropical regions in five continents. Regions where malaria occurs are, of course, restricted to those inhabited by the anopheline mosquito. Attempts to eliminate or at least suppress the disease have been an important public health story through much of the last century. For details see section 2.2.3. At malaria’s furthest reaches, in temperate zones characterized by strong seasonality and cold winters, these attempts have been successful. Beyond any other factors, this reflects the fact that the base case reproduction rate of malaria (parasite and vector) is considerably lower in temperate regions than in the tropics, so that moderately intensive efforts at vector control and case management can lead to elimination of the disease. The remarkably high transmission rates in sub-Saharan Africa also reflect the particular capacity of Africa’s main vector mosquitoes, the Anopheles gambiae complex of species, with their remarkable tendency towards human biting (anthropophily). For details see section2.1.These climatic patterns reflect the natural history of the disease. The malaria parasite is transmitted to the female Anopheles mosquito from an infected individual when it takes a blood meal as a prelude to the reproductive process. The parasite develops within the mosquito before it becomes infectious to other individuals in the course of subsequent blood meals. For details of the reproduction cycle see section 2.1.1. The period required for that life-cycle change increases as the ambient temperature declines, and given the life span of the mosquito, transmission becomes much less likely when the temperature falls below 18°C. Moreover, malaria parasites cease development completely at temperatures below 16 °C, and many species of vector mosquitoes suspend biting activity at very low temperatures, further reducing the stability of malaria transmission in temperate regions.
Although other climatic features such as rainfall and humidity also affect the stability of transmission, seasonal temperature variation is a predominant factor in explaining the geographical distribution of the disease. Cold winters and moderate temperatures in summer facilitated effective elimination of malaria infection from much of the temperate zone . In tropical regions, exposure to mosquitoes may be perennial and frequently includes several contacts with infected vector mosquitoes each night. Such inoculation rates, combined with the long duration of parasite survival in the mosquito , rapidly saturate local human populations, resulting in universal prevalence and superinfection. This stable pattern of transmission resists amelioration, and vector control efforts that succeed in temperate zones have repeatedly failed to eradicate the parasite from tropical and subtropical regions, although control is possible[99].
illustration not visible in this excerpt
Figure 5: Global Distribution of Malaria (Source: [99])
The changing global distribution of malaria risk from 1946 to 1994 shows a disease burden that is increasingly being confined to tropical regions. The changing global pattern of malaria transmission from 1946 to 1994 illustrates the success of anti-malarial efforts in the more temperate regions of the world and the increased concentration of disease burden in the tropics (Source: [99])
2.3. 2 Prevalence and Incidence
This section is mainly taken from the incidence and prevalence database , status February 2004[44]and WHO fact sheet no 94, revised October 1998[122]. Further quotations are indicated.
There have been several attempts to quantify malaria’s importance epidemiologically during the last decade with increasing interest in controlling malaria through strengthened national and local health care systems. Estimates have remained for the most part close to the often quoted figure of 1 million de a ths and the number of cases and infections has varied from 30 0 to 500 million. Most importantly, there has been a general consensus that about 90% of all cases occur in Africa, although the basis for this assumption has not been clear. Relatively few reports of economic toll due to malaria have been published. About 93% of the 550 million people living in Africa are at risk of malaria.
A recent study shows that in the 1990s 26% of the more than 1500 children born in 1990 in rural western Kenya died over a fou r-year period. Neonatal and infant mortality were 32 per 1000 and 176 per 1000 live births respectively. In Africa, malaria-attributable death rates have been reported as high as 25% to 30% for children under the age of 5 years. These rates, based often on the change in mortality following intervention projects drop below 5% in children over age of 5 years in areas of stable endemicity. If these figures can be generalized up to 2 5% or more of all African children born in malarious areas will die from malaria. Malaria’s burden reflects the variability in the microepidemiology of the disease and the availability and effectiveness of control measures throughout the continent.
Malaria-related effects on pregnant women, their fetuses and newborns comprise an ext remely large and often hidden burden. Malaria causes up to 15% of maternal anemia and some 35% of low birth-weight episodes. Between 75,000 and 400,000 infant deaths per year are associated with malaria infections during pregnancy.
Close to 600,000 persons contract cerebral malaria yearly, with a case fatality rate of about 20%. Neurologic complications lastin g longer than 6 months occur in up to 19,000 of these patients. Severe anemia occurs in 1.5 to 6.0 million African children; with a case fatality rate of nearly 15% up to 1 million children may die every year from malaria-induced anemia. Respiratory Distress , hypoglycemia and overlapping conditions contribute another 1 to 2 million cases and with a mortality rate nearing 20% well over 200,000 deaths. In Africa, there may be up to 1 million malaria-associated low birth weight babies born each year and about 400,000 of these children will die. All of these events contribute up to 1.7 million deaths in African children yearly.
Many travelers visit so-called “risk areas”, and cases of malaria acquired by international travelers from industriali z ed countries probably number 25,000 to 30,000 annually; of these 10,000 are reported, the numbers of P. falciparum malaria being as much as up to 8,000 per year, and 150 malaria cases are fatal[14], [98], [117].In the USA, 1245 malaria cases have been reported in 2002 compared to 1544 in 2001. In the former USSR, the reported annual incidence dropped from 1145 in 1989 to 356 in 1990 after cessation of the activities in Afghanistan.
Because there is a significant lack of surveillance data on imported cases of infectious diseases in Europe, the E urope a n Network on Imported Infectious Disease Surveillance was founded in February 1999 as an electronic network of clinical sites related infectious diseases. The network appears to cover about 10% of all patients with malaria seen in Europe.
In The Americas 21 countries and territories report a total of more than 1 million cases of malaria per year. This is an increase from the 270,000 cases reported in 1974 and the 600,000 in 1980. The annual malaria rate is about 156 per 100,000 inh abitants. More than 280 million people are at risk, i.e. 40% of the population in malarious or potentially malarious areas. Brazil and the Andean countries report the highest number of malaria cases. In the Amazon basin, malaria is brought to indigenous people by the incursions of commercial and pioneering activities[16].
In the Eastern Mediterranean region, 240 million out of 400 million people are at risk with 10 million cases and 100,000 deaths per year.
In South East Asia and the Indian subcontinent , the malaria situation has remained stable since 1983 with the incidence of malaria between 2.5 and 2.9 million cases annually. Forest-related malaria represents 30% to 80% of the total cases, 50% to 90% of all P. falciparum malaria, and a majority of the infections with drug-resistant P. falciparum malaria. In Asia: the malaria risk is localized in certain areas whereas in Africa: the vast majority of the population is under malaria risk[97].
2.3.3 Endemicity
An answer to the question “what is a malarial epidemicity?” can be: “a sharp increase in malaria incidence among populations in whom the disease is infrequent, or an increase in clinical malaria in areas of moderate transmission constitutes an epidemic. “ Malaria epidemics occur principally in areas of low transmission, where no single age group in the population is immune. The introduction of malaria, particularly if exacerbated by changes in rainfall , long periods of increased humidity and temperature, or more permanent changes of microclimate due to the development of irrigation systems, agricultural projects or tree plantations , can trigger explosive epidemics that affect both adults and children. However, epidemics can also occur in areas of higher transmission as a result of the abandonment of control program s, immigration of non-immune people, and reduced access to treatment[1].
illustration not visible in this excerpt
Figure 6: Morbidity and Mortality in Different settings of endemicity ( Source:[46])
Several levels of endemicity are distinguished. It should be noted that the mean rates of malarial inoculation or transmission intensity are not included in the definition of any of the above mentioned types of malarial endemicity. High or low transmission rates can occur for stable, unstable and endemic malaria[46].
2.3.3.1 Stable Endemic Malaria
Stable endemic malaria occurs when a population is continuously exposed to a fairly constant rate of malarial inoculation.
Due to the regularly delivered inoculations, a strong protective immunity against overt illness and risk of death is acquired, usually b y the age of 4 or 5 years (“partial immunity” because infected individuals still fall sick) . Before this age, there is much morbidity and mortality especially in the presence of P. falciparum malaria. Such conditions mainly prevail in sub -S aharan Africa. The age-dependent pattern of immunity to malaria inthe endemic parts ofAfrica is often attributed to the intense malaria transmission rates in this region. There is a clear shift from severe malarial disease in younger children (<5 years of age) toward relatively increased rates of both mild and severe disease in older age groups at EIR probably below 10 to 20 infectiouosbites per year[16].
2.3.3.2 Unstable and Epidemic Malaria
Unstable endemic malaria occurs when a population is subjected to more or less permanent malaria transmission but under circumstances in which there are large fluctuations in the rates at wh i ch malarial inoculations are delivered to individuals within the population. Epidemic malaria is an extreme form of unstable malaria . It occurs when a population is subjected to an increase in malaria transmission rates above that previously or normally experienced. When P. falciparum is involved malaria epidemics can be among the most lethal forces of nature[16].
Where transmission conditions are unstable, low to moderate malaria inoculation rates can be highly dangerous. This is because partial immunity to malaria while slowly gained is rapidly lost following half a year to a year without infection. Wherever the rate of delivery to malarial inoculations is both low and highly erratic over extended periods of a year the risk of eventual reinfection remains high. In these circumstances individuals are vulnerable through life to clinically active malarial infection. All species of malaria parasite become dangerous under these circumstances. Life expectancy can be reduced to half or less of that in a contemporary malaria-free and otherwise infect ive envir o nment. With no anti-malarial immunity, populations at the margins of malaria transmission zones are vulnerable to epidemic malaria. Similar and even higher malaria mortality rates were experienced by Europeans entering tropical regions before the introduction of quinine in the mid-19th century[16].
2.3. 4 Epidemic preparedness, prediction and prevention of epidemics
When an epidemic occurs, the urgency for action seldom allows enough time for planning and implementing the necessary control measures, unless there is an adequate degree of preparedness. In epidemic-prone areas, this preparedness should come from an appropriate prediction system based on monitoring epidemic risk factors. Epidemic and emergency preparedness is being promoted as an essential activity of health services. In line with this, WHO is supporting the organization and work of inter - country emergency preparedness teams in Africa which will collaborate with affected countries. In epidemic-prone areas, it is essential that a close collaboration is established between the specialized anti-malarial services and the emergency preparedness teams. The specialized services could then assist in the:
-identification of epidemic-prone areas, the main risk factors and alarm signals
-monitoring of risk factors
-planning, implementation and evaluation of preventive or control measures, taking into account essential epidemiological characteristics (e.g. parasite sensitivity to drugs and vector susceptibility to insecticides)[120].
The concept of risk detection should be considered in relation to the time available for implementing an appropriate response. After recognizing an imminent epidemic risk, it is particularly important to be able to estimate the potential magnitude of the forthcoming epidemic wave, as well as the area of potential spread[120].
2.3. 5 Epidemiological information systems
Information systems have often been designed to provide managerial and epidemiological data thought necessary to monitor the impact of interventions and the implementation of control program activities. Renewed interest in malaria epidemics has made malariologists and epidemiologists aware of the fact that most epidemics are caused or greatly influenced by meteorological or socioeconomic determinants. However, most anti-malarial services have still not set up mechanisms to monitor these variables. It is essential that health services have the epidemiological competence to select suitable indicators and the capacity to coordinate inter - sectoral collaboration to monitor them in time[120].
An essential component of any epidemiological information system is an appropriate geographical information system. As epidemics are catastrophic events, their study requires precise definition of time and location. For both the implementation of control interventions and understanding of risk dynamics, it is necessary to define the geographical limits of each epidemic as much as possible. As most malaria epidemics are the result of abnormal meteorological conditions, climate monitoring will provide the most useful indicator of epidemic risk. Analysis of past records will permit the identification of alarm signals (e.g. early and prolonged rains, floods and monsoon failures), which could alert the epidemic preparedness system to prepare an adequate response[120].
Epidemics resulting from environmental modifications or social disturbances will require the continued alertness of malaria epidemiologists to the social and economic conditions in malarious or potentially malarious areas[120].
Early detection of epidemic situations requires a definition of normality. The most practical method is the determination of epidemic indices by plotting the median and the third quartile of the malaria incidence (or merely the numbers of malaria cases) every calendar month of previous years. This defines a normal range on which to plot the current data in order to detect an abnormal increase. Malaria program s should support district medical officers to ensure that at least a few health facilities (hospitals and health centers ) in epidemic - prone areas adopt this method of epidemiological analysis[120].
2.3. 6 Resistance Pattern
Resistance of P. falciparum to CQ is now common in practically all malaria-endemic countries of Africa (Fig.2), especially in east Africa, thus posing increasing problems for the provision of suitable treatment. As a consequence Malawi and Kenya, in 1993 and 1996 respectively, changed their recommendations for first-line treatment of uncomplicated malaria from CQ to sulfadoxine/pyrimethamine (SP) , and Botswana and South Africa revised their treatment guidelines in 1997. Kenya reports treatment failures with SP . Increased gametocyte prevalence and density after SP treatment failure may increase the spread of SP-resistant strains in the population[9].No CQ resistance has been reported from Central America west of the Panama Canal, the island of Hispaniola (Haiti and the Dominican Republic) and cert a in areas of the middle east. Resistance to SP , the main alternative to CQ , is widespread in south-east Asia, south Asia, sub-Saharan Africa, Oceania and South America (mainly Amazon basin). Recent reports from Kenya and the United Republic of Tanzania suggest that changes in parasite susceptibility to SP have occurred and may presage clinical resistance. Mefloquine resistance is now common in the border areas of Thailand with Cambodia and Myanmar. Parasite sensitivity to quinine is declining in several other countries of south-east Asia and in the Amazon region, where it has been used in combination with tetracycline for the treatment of uncomplicated malaria. Consequently, artemisinin and its derivatives are now increasingly being used as first-line treatment in some of these areas. Resistance of P. vivax to CQ has now been reported from Oceania including Indonesia (Irian Jaya), Myanmar, Papua New Guinea, Vanuatu and the Solomon Islands as well as India, Thailand, Myanmar and South America including Brazil, Guyana and Peru. Cross-resistance to amodiaquine sometimes occurs. Strains of P. vivax that are tolerant or even resistant to primaquine are found in areas of Southeast Asia and East Africa including Somalia. An increasing number of malaria epidemics have been recently documented throughout the world, particularly in Africa[6],[98].For further details and therapeutic approaches see section 3.2.
In absence of a firmly established gene responsible for CQ and amodiaquine, resistance in Plasmodium falciparum surveillance to these first-line treatments in Africa needs to be performed in vivo or in vitro. In vivo(animal models)and in vitro tests can be discordant due to immunity status and low plasma levels (wide inter - individual variations of pharmacokinetics in particular plasma levels)[6].
Genotyping of pre-treatment and post-treatment isolates should be done via polymerase chain reaction (PCR) in order to distinguish between recrudescence and reinfection[6].
illustration not visible in this excerpt
Figure 7: Global malaria status (source:[120])
illustration not visible in this excerpt
Figure 8: Drug-resistant malaria and pesticide-resistant mosquitos (source:[120])
2.3.7Travelers
Although tropical diseases are not endemic in the Western World, the rise in international tourism and economic migration has meant that more people from developed countries are now at risk from infection. The principal reporting countries are France, Germany, Italy and the United Kingdom. For detailed numbers see section 2.3.2. Undoubtedly, awareness of the seriousness of tropical diseases, previously thought to be of low priority, has risen. This has created renewed demand for effective pharmaceuticals for use in the traveling population and military personnel. The overall incidence figure is growing. U rban areas, mainly populated by new immigrant populations, are also becoming significant target populations for treatments directed to diseases, such as malaria. The developed world travel market has been tapped, to some extent, by manufacturers marketing products to prevent common tropical infections, most notably vaccines but also malarial chemoprophylaxis. Travel to exotic locations, such as Africa and Asia, from developed nations has increased in recent years. This reflects the increasing potential for pharmaceuticals targeting diseases endemic to less developed regions, not only in those regions, but also in more affluent Western markets[112].
Theincreased international travelis in line withan increased risk of transmission in areas where malaria control has fadedand wheredrug-resistant strains of Plasmodiae, especially P.falciparum are widely spread.Without chemopropyhlaxis, a traveler’s risk is highest in areas of Oceania (>20% per month) and in sub-Saharan Africa (2% per month). Most cases occur after travel to Africa (40-50% of reported malaria cases) and the South Asia-Indian subcontinent region ( 25% of the cases)[14],[98], [117].
Malaria can present months or even years after travel. Of the cases reported in the United States, approximately 40% to 50% involve infection with P. vivax, 35% to 45% are due to P. falciparum, 4% are caused by P. malariae, 2% to 3% are due to P. ovale, approximately 5% involve unknown species and less than 1% are due to multiple species[98].
Malaria in travelers is largely preventable: most occurrences are due to inadequate or incorrect pre-travel advice or lack of compliance with a recommended chemoprophylactic regimen. Drug resistance is also in creasingly being recognized as a contributing factor. In the United States, mortality from malaria is approximately 4% increasing to 30% in individuals older than 70 years of age[98].Chemoprophylaxis and other preventive measures continue to provide effective protection against malaria for the 30 million travelers who visit regions where malaria is endemic every year. Still, there is room for improvement in prophylactic regimens and in the diagnosis and treatment of travelers’ malaria when it occurs[14], [117].
Another issue are areas where there is civil unrest or other conflicts[97](not an issue for travelers).
2.4Malariain the Pediatric Population and Pregnant Women
Immunity to malaria develops over several years of almost continuous exposure and infection. It is characterized by a gradual decrease in the frequency and severity of clinical disease. Repetitive waves of antigenic variation may account for this gradual ons e t of immunity[98].Asymptomatic infections are common.
In all endemic regions, children and pregnant women are the two groups mostly at risk of severe disease and death[73].Malaria is the leading cause of mortality among children <5 years of age in Africa and is the cause of approximately 20% of all-cause mortality in this age group[129].Although older children have developed some degree of immunity the disease remains one of the most common causes of school absenteeism in these areas[105],[122].
2.4.1PediatricPopulation
Usually, in the first two months of life, children may not contract malaria or the manifestations may be mild with low-grade parasitemia, due to the passive immunity offered by the maternal antibodies.
In case the maternal immunity has not been effective, a congenital malaria infection can have the symptoms of fever, jau n dice, anemia and hepatosplenomegaly late in the first month or during the second month of life. These children usually respond to standard anti-malarial treatment. Fewer than 7 to 10% of infected children are actually becoming ill with malaria. It seems that many children clear their ma ternal infection spontaneously. Passive immunity due to maternal antibodies, retarded growth of the parasites in erythrocytes containing hemoglobin F and resistance for parasite growth in old red cells with HbF may be the causes. Nonetheless, some children get sick with their congenital malaria[27].
Newborns can be infected and sick with their own malaria infection. As a result of this, many children are born with low birth - weight (they are not born with their own infection but suffer from their mothers ’) . Others suffer from anemia and increased rates of malaria in the early months of life. It is estimated that approximately 6% of all infant deaths in malaria-endemic areas of the world are a result of malaria infection that took place during the child ’s prenatal life[32].
Many factors influence a patient’s risk to develop malaria, particularly the species of malaria parasite and the patient’s immune status which depends on previous exposure to malaria. In areas of high intensity malaria transmission, most mortality occurs among young children as a result of severe malaria in immunologically naive patients. In the same population, infected adults and older children may have minimal symptoms or may be asymptomatic due to acquired immunity[110].
Studies show that the risk of morbidity declines rapidly with age, such as children aged 5 to 9 years experience between 0.25 and 2.3 malaria attacks per annum (p.a.) and children aged 10 to 20 years experience between 0.1 and 1.3 attacks p.a[10].
The commonest and mo s t important complications of P. falciparum infection in children are cerebral malaria, severe anemia, respiratory distress and hypoglycemia (hyperlactatemia) . For details see section 2.1.2. Differences between severe malaria in adults and children are highlighted in the following table.
illustration not visible in this excerpt
Table 2: Signs and Symptoms of severe malaria in adults and children ( Source:[58])
Children with malaria can in most cases be quickly and effectively treated with a course of inexpensive oral tablets. But because fever may be the only sign of malaria it may be difficult to distin guish it from other potentially life-threatening conditions[121].
2.4.2Pregnant Women
Malaria infection during pregnancy is a major public health problem in tropical and subtropical regions throughout the world. In most endemic areas of Africa, pregnant women are the main adult risk group for malaria. This is probably due to, or at least in part, the “immunosuppressed” status of the pregnant woman. Even in otherwise highly malaria-immune women, the risk of malarial infection in pregnancy is high with increased risk of low birth weight, miscarriage, infant mortality and morbidity / mortality in the pregnant woman[16],[32].
The natural immunosuppression of pregnancy and the pre-partum level of immunity are important determinant s of disease severity. The notion that the placenta is an “immunologically privileged site” (like the eye, brain and testes) has been used to account for the localization of parasites there; i.e. ef f ector mechanisms operating elsewhere in the body which kill the parasites do not operate in the placenta. Pregnant women with severe malaria have an increased risk of pulmonary edema and hypogl y cemia which means pregnant women are particularly vulnerable to quinine-stimulated hyperinsulinemic hypoglycemia[119].
The main burden of malaria infection during pregnancy results from infection with P . falciparum. The impact of the other three human malaria parasites (P. vivax, P. malariae, and P. ovale) is less clear. Every year at least 30 million women in malarious areas of Africa become pregnant; most of these women live in areas of relatively stable malaria transmission. The symptoms and complications of malaria during pregnancy differ with the intensity of malaria transmission and thus with the above mentioned level of immunity acquired by the pregnant woman. Since malaria transmission intensity may vary within the same country from areas of relatively stable transmission to areas of unstable or epidemic transmission, the clinical picture of malaria infection during pregnancy may likewise range from a symptomatic to severe, life - threatening illness[1], [4], [73],[119].
In areas of epidemic or low (unstable) malaria transmission, adult women have not acquired any significant level of immunity and usually become ill when infected with malaria, the severity of the disease usually being higher than in non-pregnant women . For pregnant women in these areas the risk of developing severe malaria is 2–3 times higher than that for non-pregnant women living in the same area. Maternal death may result either directly from severe malaria or indirectly from malaria-related severe anemia. Early detection and prompt treatment with anti-malarial drugs are essential to reduce mortality. In areas of high and moderate (stable) malaria transmission, most adult women have developed sufficient immunity that, even during pregnancy, P. falciparum infection does not usually result in fever or other clinical symptoms. Adverse effects are largely confined to the fetus of the first pregnancy. In these areas, the principal impact of malaria infection is malaria-related anemia in the mother and the presence of large numbers of mature parasites and abundant pigment in the placenta. The resulting impairment of fetal nutrition contributes to low birth weight (approximately 170g less ) and is a leading cause of poorer infant survival and development. In areas of Africa with stable malaria transmission, P. falciparum infection during pregnancy is estimated to cause an estimated 75 , 000 to 200,000 infant deaths each year. Pregnant women with cerebral malaria have a case-specific mortality rate o f twice that of non-pregnant adults ; f etal death is common. Despite the toll that malaria exacts on pregnant women and their infants, this was – until recently – a relatively neglected problem, with less than 5% of pregnant women having access to effective interventions[1],[4], [73] [119].
2.5 Malaria as a Disease of the Poor
Tropical infectious diseases are the biggest killer of children and young adults globally, accounting for up to five million deaths each year [89]. The majority of these deaths occur in the poor less-developed nations of Africa, Asia and South America [112]. The disparity in health status probably results largely from differential access to drugs that are already available as well as to sanitation,safe waterand housing, which influence the transmission of some diseases. The health disparity between rich and poor countries results in average life spans of 77 and 52 years respectively. Deaths attributable to tropical infectious diseases (table3)– apart from HIV -contribute most to the disparity. Deaths associated with diarrhea and respiratory infection are rare in industrialized countries but aremajor killers of children in developing countries, especially in Africa. Diseases that do not occur in industrialized countries, e.g. malaria and schistosomiasis, or ones that are comparatively rare in these countries, e.g. tuberculosis and HIV/AIDS, impose a heavy burden on both adults and children in developing countries [125]. For example, in 2001, malaria resulted in 963,000 deaths in Africa, compared to 200 deaths in Europe [89].Malaria accounts for between <3% and 8% of all reasons for school absenteeism. Of pr e ventable medical causes of absenteeism malaria accounts for a significant 13-50% of school days missed p.a[10].
The burden of morbidity from a number of untreated, debilitating but rarely fatal diseases in developing countries, including sexually transmitted infections, has a substantial impact on productivity. An analysis of the differences in the disease burden between the poorest and the richest 20% of the world’s population suggested that, in 1990, nearly 80% of the difference between the poor and rich in terms of death and disability-adjusted life years was attributable to communicable diseases. This is still likely to be true, as the incidences of HIV, malaria, and tuberculosis are increasing. Furthermore, the aging of the population in the developing world can be expected to bring increases in the absolute burden of non-communicable disease [50], [125].
illustration not visible in this excerpt
Table 3: Deaths attributable to infectious diseases by region, 2001(Source:[89])
There is a clear variation in geographical incidence tropical infections. Disease incidence in less-developed regions, such as Africa and South-East Asia, is a clear demonstration of how economic constraints / financial impossibility.(Source:[89])
As a general rule of thumb, where malaria prospers most, human societies have prospered least. The global distribution of per-capita gross domestic product (GDP) in 1995, adjusted for purchasing power, shows a striking and unmistakable correlation between malaria and poverty. Poverty is concentrated in the tropical and subtropical zones, the same geographical boundaries that most closely frame malaria transmission. The extent of the correlation suggests that malaria and poverty are intimately related. This correlation can, of course, be explained in several possible ways. Poverty may promote malaria transmission; malaria may cause poverty by impeding economic growth; or causality may run in both directions. It is also possible that the correlation is at least partly spurious, with the tropical climate causing poverty for reasons unrelated to malaria.It is certainly true that poverty itself can be held accountable for some of the intense malaria transmission recorded in the poorest countries. Personal expenditures on prevention methods such as bednets or insecticides, increased funding for government controlprograms, and general development such as increased urbanization can reduce malaria transmission.Housing is also a major factor of prevention.The elimination of malaria from wealthier countries in the 1930s to 1950s, such as the United States, Italy, Greece and Spain, was a result of both socioeconomic development and intensiveanti-malarialinterventions.For details see section 2.2.3.The causation in the other direction, from malaria to poverty, also seems to be robust and powerful. Cross-country regression analysis estimating the long-term impacts of malaria on economic growth and development suggest the significance of the economic burden of the disease. This analysis finds that countries in which a high proportion of the population lived in regions of P. falciparum malaria transmission in 1965 had annual economic growth rates that were 1.3% lower than other countries over the period 1965–1990, even after controlling for the other standard growth determinants used in macroeconomic analyses. These other determinants include levels of human capital, life expectancy, initial income, and macroeconomic policy indicators of various kinds as well as geographical factors such as tropical location that could be simultaneously influencing malaria and economic growth. Because this shortfall refers to the annual growth rate, the long-term effect on the level of gross national product (GNP) per capita is the cumulative effect of an annual reduction in growth.GNP per capita in a malarious countryisless than half of that in a non-malarious country [35], [83],[99].
[...]
- Quote paper
- Petra Heyen (Author), 2004, The fight against Malaria in Malaria-Endemic Countries, Munich, GRIN Verlag, https://www.grin.com/document/37928

Similar texts






Publish now - it's free

Comments